Legislative Update - May 15, 2024
 IHA Challenges Flawed and Outdated RAND 5.0 Report
IHA Challenges Flawed and Outdated RAND 5.0 Report
The RAND 5.0 report was released earlier this week at the National Healthcare Price Transparency Conference in Indianapolis. The report ranked Indiana 8th highest in total commercial hospital prices between 2020 and 2022. Indiana’s ranking improved slightly compared to RAND 4.0, in which Indiana ranked 7th highest; however, IHA continues to challenge the study’s validity and methodology. IHA released a statement from IHA President Brian Tabor to statewide media identifying the critical shortcomings of the RAND 5.0 report.
Every RAND report on hospital prices has relied on incomplete, outdated data, excluded hospital affordability commitments, dismissed cost pressures facing hospitals, and presented Medicare rates as an appropriate benchmark despite Medicare paying far below the cost of care. Given the current state of Indiana’s health care system, in which hospitals’ financial sustainability remains at risk, the portrait they paint could not be further from reality. IHA will continue challenging the validity of such reports and advocate for comprehensive, meaningful policies that address affordability in an effective and equitable manner.
 A Game of Political Musical Chairs: The 2024 Primary Election
A Game of Political Musical Chairs: The 2024 Primary Election
In a decisive win, U.S. Senator Mike Braun emerged quickly from a crowded field to become the Republican nominee for Governor. Six candidates, including current Lieutenant Governor Suzanne Crouch and former Indiana Secretary of Commerce Brad Chambers, were in the race that concluded last Tuesday. About 24 hours after winning the Republican primary, Senator Braun announced that State Representative Julie McGuire is his preferred running mate to lead the next state administration. In a news release, Braun stated, “Julie shares my vision of making Indiana a national beacon of freedom and opportunity, and I’m proud to have her on the team.” Although Representative McGuire is Senator Braun’s preferred candidate, she will still face competition to become the Republican nominee for Lieutenant Governor during the party’s stat convention this summer. In Indiana, the party’s nomination for the position has to be approved by delegates from around the state during the party’s convention and Representative McGuire currently has one opponent for the bid - Micah Beckwith, a pastor in Hamilton County with a growing conservative following. Senator Braun will face off against Democrat Jennifer McCormick, former Indiana Superintendent of Public Instruction, in the November general election to determine who will serve as Indiana’s next governor.
Several retirements from the Indiana General Assembly made for a very interesting primary for candidates looking to serve in the Statehouse. In the House of Representatives, there were eight open seats due to retirements and 26 contested races in total. State Representative Chuck Goodrich, who announced he would vacate his seat to run for Congress, was unsuccessful in his challenge to incumbent Congresswoman Victoria Spartz, even though Spartz had previously announced she would not seek re-election before abruptly rescinding that commitment and running. Alaina Shonkwiler, a former district director for Spartz, was victorious in securing the Republican nomination to fill the seat vacated by Goodrich. Shonkwiler now faces Democrat Christopher Hartig for the seat. In House District 24, covering parts of Boone and Hamilton Counties, State Representative Donna Schaibley’s retirement opened the door for a Republican primary victory for Hunter Smith, former Colts punter. Republican Tonya Isa was able to pull off a victory in northeast Indiana’s House District 51 due to the retirement of Representative Denny Zent. The only retirement in the Senate was John Crane from Avon, which led to a victory for Brett Clark, Navy veteran and former Hendricks County Sheriff in the Republican primary for Senate District 24, covering parts of Hendricks and Putnam counties. Even after the primary, retirements are impacting the future makeup of the Indiana General Assembly. State Representative Rita Fleming, a retired physician from southern Indiana, announced her retirement a week after the primary, so the Indiana Democratic Party will hold a caucus to select her replacement.
The future makeup of Indiana’s congressional delegation was not immune from changes either. In the primary for the Third Congressional District, voters selected a familiar face, Marlin Stutzman, who held the seat from 2010 to 2017 to seek election to the position vacated by current Congressman Jim Banks, who walked away from Tuesday as the Republican nominee for the U.S. Senate seat left open by Mike Braun due to his candidacy for governor. Stutzman will go up against Democrat Kiley Adolph in the general election. Additionally, in the wake of Congressman Larry Bucshon’s announcement to retire from his position representing the Eighth Congressional District, we saw State Senator Mark Messmer win the primary to be the Republican nominee for the open seat. Messmer will face Democrat Erik Hurt, who defeated three others in the primary, in November.
The Friends of Indiana Hospitals Political Action Committee remains engaged and will continue to prioritize the hospital industry’s best interests in such an active political environment. If you have any questions about races not covered here, please do not hesitate to reach out to IHA’s Government Relations team.
 Interim Study Committee Topics Assigned
Interim Study Committee Topics Assigned
The Indiana General Assembly’s Legislative Council convened Tuesday, May 14 to approve various procedures and topics to be studied during the legislative interim. Interim Study Committees, which are comprised of members of both the House and Senate, meet throughout the summer and fall to study the issues assigned to them, the work product of which often informs legislative proposals in the upcoming session, which for 2025 will begin in January and adjourn by the end of April. The Interim Study Committee
topics assigned for the 2024 interim can be found here, and highlights are as follows:
Interim Committee on Public Health, Behavioral Health, and Human Services:
-
Approval of agreements with private attorneys and private entities when the Child Support Bureau determines that a reasonable contract cannot be entered into with a prosecuting attorney to administer the child support provisions of Title IV-D of the Federal Social Security Ac
Health Care Cost Oversight Task Force:
-
Oversight of health care costs.
-
Review corporate practice of medicine.
Medicaid Oversight Committee:
-
Review, consider, and make recommendations concerning the Medicaid program.
Legislative Update - March 29, 2024
2024 Legislative Session Adjourned
 The 2024 legislative session adjourned for the year on Mar. 8, earlier than the statutory adjournment deadline of Mar. 14, resulting in an even quicker “short session” as legislative leaders predicted. IHA brought forth a wholistic plan to modernize the state’s Hospital Assessment Fee to leverage all available federal funds at the outset of the legislative session, but following an unexpected Medicaid shortfall in December, legislative leaders conveyed their desire to wait until the 2025 legislative session for a comprehensive Medicaid redesign. The 2025 legislative session will be a long, budget-writing session, in which hospital base rates will also be reviewed. IHA looks forward to working with legislative leaders, the Indiana Family and Social Services Administration, and IHA’s members on the redesign throughout the remainder of the year heading into the 2025 legislative session.
The 2024 legislative session adjourned for the year on Mar. 8, earlier than the statutory adjournment deadline of Mar. 14, resulting in an even quicker “short session” as legislative leaders predicted. IHA brought forth a wholistic plan to modernize the state’s Hospital Assessment Fee to leverage all available federal funds at the outset of the legislative session, but following an unexpected Medicaid shortfall in December, legislative leaders conveyed their desire to wait until the 2025 legislative session for a comprehensive Medicaid redesign. The 2025 legislative session will be a long, budget-writing session, in which hospital base rates will also be reviewed. IHA looks forward to working with legislative leaders, the Indiana Family and Social Services Administration, and IHA’s members on the redesign throughout the remainder of the year heading into the 2025 legislative session.
End-of-Session Overview
 Read the overview of bills enacted this session in IHA’s full 2024 Legislative Session Report. Items of note include:
Read the overview of bills enacted this session in IHA’s full 2024 Legislative Session Report. Items of note include:
- Reinstatement of the ability of the Indiana Department of Health to grant time extensions for hospital fiscal reports (HEA 1259 and
SEA 132).
- Additional flexibility for clinical nurse preceptors and nursing program faculty (HEA 1259).
- Additional pathways for foreign-educated nurses to become licensed in Indiana (SEA 132).
- A study of emergency medical services across Indiana so recommendations may be provided to the Indiana General Assembly ahead of the budget session (HEA 1302).
- The repeal of the requirement that out-of-state practitioners must provide the Indiana Professional Licensing Agency a certification to practice telehealth in Indiana (SEA 132)
- Updated language that ensures Medicaid reimbursement for individuals under emergency detention orders (HEA 1216).
There were several bills that did not make it across the finish line as well, following IHA’s advocacy due to their harmful provisions. Items of note include:
-
HB 1200, which would have imposed price caps for the State Employee Health Plan;
-
HB 1327, which would have created new ownership reporting requirements on hospitals;
-
HB 1414, which would have allowed Medicaid-managed care organizations to pay below the Medicaid rate; and
-
SB 168, which would have created additional 340B program reporting.
Legislative Update - March 1, 2024
 Mergers and Acquisitions Legislation Moves Closer to Final Passage
Mergers and Acquisitions Legislation Moves Closer to Final Passage
Earlier this week, the House passed
Senate Bill 9 which requires certain mergers and acquisitions between health care entities to be reported to the Attorney General's office. The bill was sent back to the Senate as a motion to concur with the amendments adopted by the House Public Health Committee. Early next week, the full Senate will consider whether they agree with the changes. IHA remains opposed to the legislation and still contends that the current federal framework, which is currently being strengthened through the FTC, is adequate and protects consumers. The current federal process has safeguards built in that ensure the review does not negatively impact a community's access to health care. IHA continues to advocate for further changes to be made before the motion to concur is voted on next week. IHA is in communication with relevant lawmakers and will provide an update next week on whether that happens.
 Senate Terminates Ownership Disclosure Bill and Keeps LARC Alive
Senate Terminates Ownership Disclosure Bill and Keeps LARC Alive
The Senate Health and Provider Services Committee decided not to consider
House Bill (HB) 1327 this week. The bill would have required health care entities to report ownership information to their respective regulatory bodies and would have required insurers to provide the employer consumers with specific claims data. This week's committee hearing was the last chance to consider the bill, therefore it is dead. However, language from the bill is still eligible to be amended into another bill through a conference committee so IHA will continue to monitor.
HB 1426, which requires hospitals to offer long-acting reversible contraceptives to Medicaid patients and requires the Family and Social Services Administration (FSSA) to ensure reimbursement is provided if such services are delivered, was amended by the Senate Appropriations Committee this week. The amendment adopted by the committee sunsets the bill's requirements on June 30, 2025, then requires the FSSA to explore available federal funds to use for such services going forward. The bill will now head to the full Senate for further consideration.
 Workforce and Fiscal Report Bill Heads to Governor's Desk
Workforce and Fiscal Report Bill Heads to Governor's Desk
The Senate voted to approve amendments adopted in the House on
Senate Bill (SB) 132 this week. The bill includes various professional occupation provisions, specifically allowing foreign-educated nurses to benefit from all avenues to become licensed in Indiana, which builds on IHA’s efforts from 2022 under the ‘Nursing Indiana Back to Health’ initiative. Additionally, IHA was successful in advocating for language to reinstate the ability for hospitals to obtain extensions granted by the Indiana Department of Health to the deadline for submitting annual fiscal reports. Last year, under House Enrolled Act (HEA) 1004, such deadline extensions were prohibited, so we are pleased to report this language will be reinstated for necessary flexibility in submitting fiscal reports. The bill now heads to the Governor for his signature.
Legislative Update - February 23, 2024
 IHA Announces Pledge to Support State’s Health First Indiana Initiative
IHA Announces Pledge to Support State’s Health First Indiana Initiative
Hundreds of public health advocates gathered earlier this week for Public Health Day hosted by the Indiana Department of Health to promote the importance of public health in Hoosiers’ lives and raise awareness of current initiatives to improve the delivery of services around the state. Steve Holman, Union Health CEO, and 2024 IHA Board Chair, presented to the group and publicly announced IHA’s pledge to support the State’s Health First Indiana initiative. Holman stated, “IHA and its member hospitals are fully committed to partnering with our state and local health leaders to ensure each and every Hoosier has access to the critical services they need to achieve their highest quality of life. This is our opportunity to improve the health of our citizens and the overall delivery of care in communities large and small across the state.” Vanessa Green Sinders, President and CEO of the Indiana Chamber of Commerce also presented the case for improving public health services as a factor in keeping Indiana’s business climate competitive. During the event, the Indiana Department of Health recognized Representative Brad Barrett (R-Richmond) and Senator Ed Charbonneau (R-Valparaiso) who played a crucial role in launching these initiatives through Senate Enrolled Act 4 last session. IHA is grateful for their efforts and stands ready to build on these partnerships to ensure Indiana is in the best possible position to improve the health of every Hoosier. Read the
IHA press release.
 Senate Considers Long-Acting Reversible Contraceptives and Employers’ Access to Claims Data
Senate Considers Long-Acting Reversible Contraceptives and Employers’ Access to Claims Data
Earlier this week, the Senate Committee on Health and Provider Services voted to approve
House Bill 1426 which requires hospitals to offer long-acting reversible contraceptives to Medicaid patients and requires the Family and Social Services Administration to ensure reimbursement is provided if such services are delivered. The bill was recommitted to the Senate Appropriations Committee due to its fiscal impact on the State and we are unsure it will survive due to the scrutiny given to Medicaid expenditures currently. In addition to HB 1426, the committee considered
HB 1327 which requires health care entities to report ownership information to their respective regulatory bodies and requires insurers to provide employer consumers with specific claims data. That bill was held without a vote in order to address the ownership disclosure requirements through an amendment next week. IHA is engaged on this issue and will continue working with the bill sponsor and committee members on a favorable amendment.
 Merger and Acquisition Notification Bill Moves Forward
Merger and Acquisition Notification Bill Moves Forward
Earlier this week, the House Public Committee voted to approve
Senate Bill 9 which requires certain mergers and acquisitions between health care entities to be reported to the Attorney General’s office. The bill was then engrossed on second reading by the full House on Thursday which means it will up for its third and final vote in the House on Monday. IHA testified in opposition to the bill in committee as we still contend that the current federal framework, which is currently being strengthened through the FTC, is adequate and protects consumers. The current federal process has safeguards built in that ensure the review does not negatively impact a community's access to health care. IHA will continue to advocate against this legislation and provide updates as session continues.
Legislative Update - February 16, 2024
 Health Care Workforce Legislation Continues to Move
Health Care Workforce Legislation Continues to Move
House Bill (HB) 1259, which builds upon the efforts of IHA's “Nursing Indiana Back to Health" initiative through House Enrolled Act (HEA) 1003 in 2022, was approved by the Senate Health and Human Provider Services Committee this week. It is no secret that Indiana, like all other states, is suffering from a shortage of nurses, and IHA applauds efforts such as HB 1259 to take steps to address this crisis. It is estimated that Indiana will need an additional 5,000 nurses by the year 2031 which means an additional 1,300 nurses would need to enter the workforce annually by then. The bill specifically streamlines the licensure process for foreign-educated nurses by allowing them to benefit from the licensure pathways improved by the legislation passed in 2022. The bill now moves to the full Senate for further consideration and IHA expects continued support for the measure.
 Insurance Payment for Ambulances Still Being Deliberated
Insurance Payment for Ambulances Still Being Deliberated
Earlier this week, the Senate Committee on Insurance and Financial Institutions approved a measure aimed at ensuring insurance companies pay for ambulance services at an appropriate rate. The bill,
HB 1385, authored by Representative Brad Barrett (R-Richmond) and sponsored by Senator Tyler Johnson (R-Leo), would require insurance companies to pay out-of-network ambulance service providers at any rate set by local ordinance within the municipality in which the transport begins or, absent such rate, 400% of Medicare for such services, whichever is less. A study completed by the Rural Health Research and Policy Centers shows that half of Indiana's counties contain what are known as “ambulance deserts" which means individuals live more than 25 minutes from an ambulance station. The committee adopted an amendment removing the state employee health plan. The IHA advocacy team continues to monitor this and communicate with the author and sponsor to ensure this legislation will not negatively impact arrangements between hospitals and ambulance service providers.
 Psilocybin Legislation Receives Committee Approval
Psilocybin Legislation Receives Committee Approval
This week, the House Public Health Committee voted to approve a measure that would allow Indiana to look further into the possible benefits of psilocybin on various mental health conditions. SB 139, authored by Senator Ed Charbonneau (R-Valparaiso), would establish the therapeutic psilocybin research fund to provide funds for research and require those receiving funds to conduct clinical studies and then report to the Interim Committee on Public Health, Behavioral Health, and Human Services for further review. The institutions selected to conduct such trials under this legislation would focus on research on psilocybin's effectiveness at treating conditions such as post-traumatic stress disorder, anxiety, depression, bipolar disorder, chronic pain, alcohol use disorder, and tobacco use disorder. Committee members discussed many issues, including the flexibility provided by the federal government in allowing such research to take place which they believe is an important step before legalizing or decriminalizing the substance. Additionally, one committee member raised the issue of cost and whether the steps taken to study and regulate would increase the cost of the treatment should it be permitted. The bill now heads to the full House for further consideration.
Legislative Update - February 9, 2024
Legislature Reaches Session Halftime
This week marks the halfway point of the 2024 legislative session. All bills have made their way through their chamber of origin: Senate bills through the Senate, and House bills through the House. If a bill has not been voted on in its chamber of origin by this point, it is considered "dead" and will not advance further.
However, there is an opportunity for language from dead bills to be revived and placed into bills that are still moving via an amendment. The IHA team will continue to be vigilant in fighting against any harmful language being added to bills.
Out of the 297 bills that were introduced in the Senate this session, 110 passed with 88% receiving bipartisan support and 58% receiving unanimous support. In the House, 111 bills passed out of 442 filed.
A helpful tool for determining whether bills are still working through the process is the Indiana General Assembly website. The website provides a complete list of bills filed this session. Bills listed in blue font are still alive and going through the process. Bills that have failed to advance and are effectively "dead" are in grey font.
The IHA advocacy team will continue monitoring issues diligently in the second half of session and report developments as they become available.

Concerning Legislation Not Moving Forward
IHA is proud to announce some concerning legislation that will not be advancing out of each chamber. Most of the bills listed below not only proposed restrictions or reporting requirements that go beyond what is federally required, but also could have jeopardized a patient’s access to quality care.
Senate Bill 258 would have put in place punitive physician referral restrictions beyond what current federal law requires. Senate Bill 168 would have required an entity authorized to participate in the federal 340B Drug Pricing Program to annually report additional data to the Indiana Department of Health. This proposed legislation would have created burdensome reporting requirements inconsistent with federal requirements. Senate Bill 276
would have inconsistently duplicated several federal regulations governing the provision of charity care in hospitals.
Lastly,
House Bill 1200 would have capped prices for hospitals providing services to state employees at 200% of Medicare. As the bill was drafted and amended, it would jeopardize access to quality care for state employees including state police, prison employees, highway workers, state hospitals and health care workers, their families, and many more on the state employee health plan.
Although the above legislation is dead this session, IHA will continue to monitor these topics in case similar concepts arise in another bill during the second half of session.
 IHA’s Continues to Work with the State on HAF Modernization Proposal
IHA’s Continues to Work with the State on HAF Modernization Proposal
The first step in modernizing Indiana's Medicaid system was the introduction of
House Bill 1393, specifically looking at the Hospital Assessment Fee (HAF) program and establishing a Managed Care Assessment Fee (MCAF). The bill received its initial hearing at the end of January, and the supporters who testified answered questions from legislators who were interested in the modernization plan. Although the bill unfortunately did not receive a vote, IHA continues to work with legislative leadership and the Family and Social Services Administration (FSSA) on possible alternatives as the legislation session begins its second half.
The updated HAF program would allow hospitals to be assessed up to the federally allowable maximum to increase the overall benefit of the HAF program and protect access to quality care across the state. In addition to protecting access, our proposal will help reduce the cost shift to commercial insurance.
IHA remains committed to working with the administration and lawmakers to enact a plan to achieve our goal of improving reimbursement at no additional cost to the state.
Legislative Update - February 2, 2024
 Price Cap Legislation Stalls
Price Cap Legislation Stalls
Thanks to the advocacy efforts of IHA and its members,
House Bill (HB) 1200 was removed from consideration by the House of Representatives, therefore it is dead for this legislation session. There is still a possibility that the provisions in the bill could resurface through an amendment to another bill, but lawmakers heard your voices through our recent push to oppose the legislation. The bill would have capped prices for hospitals providing services to state employees at 200% of Medicare.
We understand that price caps are never acceptable and doing so at any level this year just means that are likely to get lowered in subsequent years. Furthermore, any type of government rate setting will immediately impact marketplace negotiations and result in a significant cost shift to other plans across the state. Although HB 1200 is dead this session, IHA will continue to monitor this topic in case similar concepts arise in another bill. IHA will also continue educating lawmakers on the dangers of using data from the
National Academy of State Health Policy (NASHP) which is deeply flawed and has been used by various advocacy groups to inaccurately characterize hospital margins to push their own heavy-handed agenda.
 Merger Notification Bill Sent to the House
Merger Notification Bill Sent to the House
This week, the Senate passed
Senate Bill (SB) 9 on third reading by a vote of 49-0 which sends it to the House for consideration. The bill was amended in the Senate Health and Provider Services Committee to now require a 90-day notice of merger or acquisition to the Attorney General's office. As we have discussed, this bill stems from a recommendation adopted by the Health Care Cost Oversight Task Force that met over the interim and reviewed a variety of topics, market concentration being one of its main focuses. IHA continues to oppose the legislation, but we are communicating with the bill's author, Senator Chris Garten, and sponsor, Representative Donna Schaibley, to improve the legislation and ensure that if it is enacted into law, it is done so in the least burdensome manner possible.
 340B Reporting Legislation Does Not Move Forward
340B Reporting Legislation Does Not Move Forward
A bill proposing new requirements for entities participating in the federal 340B drug pricing program has been removed from consideration this session as it did not receive a committee hearing in the first half. The bill, SB 168 which was authored by Senator Ed Charbonneau, would have established several new reporting requirements on covered entities that go much further than those required currently under federal law. IHA is truly appreciative of its members who voiced concern over the bill which ultimately resulted in it being removed from the committee schedule this week. The 340B program will continue to be scrutinized by policymakers, in Indiana, and across the country, so IHA will continue monitoring any movement in this area and prepare for ongoing discussions in anticipation of future proposals in this space.
Legislative Update - January 27, 2024
 House Committee on Public Health Considers IHA's HAF Modernization Proposal
House Committee on Public Health Considers IHA's HAF Modernization Proposal
The House Committee on Public Health this week heard House Bill (HB) 1393 which is the first step in modernizing Indiana's Medicaid system, specifically looking at the Hospital Assessment Fee (HAF) program and establishing a Managed Care Assessment Fee (MCAF).
IHA's Deputy General Counsel, Laura Brown, opened the testimony by explaining the updated HAF program would allow hospitals to be assessed up to the federally allowable maximum to increase the overall benefit of the HAF program and protect access to quality care across the state. In addition to protecting access, our proposal will help reduce the cost shift to commercial insurance. Others who testified in support of the bill include:
-
Matt Doyle, Gary Methodist CEO
-
Dr. Eric Fish, Schneck Medical Center CEO
-
Dr. James Porter, Deaconess Hospital
-
Julie Conrad, Eskenazi Health General Counsel
-
Dr. Rick Sasso, Indiana Spine Group President
Although the bill did not receive a vote at this hearing, legislative leadership is continuing its consideration of the plan as the legislative session continues. IHA remains committed to working with the administration and lawmakers to enact a plan to achieve our goal of improving reimbursement at no cost to the state.
In the meantime, please continue to reach out to your representatives and senators, asking them to vote “yes" on this bill. Please click the button below to send a pre-written message directly to the legislators who represent your district. Estimated time 2-3 minutes.
Here's how it works:
-
Click the red button below to open the IHA Action Center.
-
Once open, there will be a sample message drafted in the Message Body section —feel free to customize this message to reflect your individual hospital.
-
Next, fill out your contact info in the boxes below the Message Body section.
-
Once complete, hit the blue “send message" button to ensure your voice is heard. You will receive a confirmation email notifying you that your message was successfully sent and to which legislators. Note: First-time users will need to authenticate by verifying their email. Be sure to check your junk/spam if you do not see that message.

 Price Caps for State Employees Health Plan Passes out of Committee
Price Caps for State Employees Health Plan Passes out of Committee
House Bill (HB) 1200 which is legislation that would counteract the work being done to pass HB 1393, passed out of House Committee on Insurance this week with a vote of nine to four.
HB 1200 would arbitrarily set price caps for hospitals and Ambulatory Surgery Centers that care for individuals on the state employee health plan at 200% of Medicare. These price caps on reimbursement do not consider the payor mix and cost pressures, or the level of services being provided to state employees at each individual hospital. This bill would result in further cost-shifting to all other employers in the state.
Proponents of the legislation point to the limited scope of the bill, as the state employee health plan “only covers 60,000 lives," and the overall impact would be spread among hospitals. However, this would lead to an immediate cut of approximately $80 million to hospitals across the state each year.
Instead of pursuing price caps, which were debated and not pursued just last year, IHA is requesting the opportunity to partner with the State Personnel Department on their tiered network program HealthSync. This program was launched just a few years ago to incentivize state employees to schedule with preferred providers with lower visit costs through lower deductibles and lower out-of-pocket maximums.
IHA will continue working with legislators on a viable plan to reduce cost shift rather than a measure that would squeeze the proverbial balloon of health care costs. The bill will continue to be considered by the committee and IHA will update members on its status through the legislative process.
 Senate Bill 9 Passes Senate Committee on Health and Provider Services
Senate Bill 9 Passes Senate Committee on Health and Provider Services
Senate Bill 9 would require health care entities to provide notice of certain mergers or acquisitions to the office of the Attorney General.
The bill was amended to require a 90-day notice to the AG's office, but IHA contends that the current federal framework, which is currently being strengthened through the FTC, is adequate and protects consumers.
Currently, the federal process has safeguards built in that ensure the review does not negatively impact a community's access to health care. For example, if an institution is failing and a merger would otherwise save access for that community, there are processes built into the federal review.
IHA will continue to fight against harmful legislation that negatively impacts hospitals and subsequently their community's access to health care.
Legislative Update - January 19, 2024
 Senate Health Committee Passes Prior Authorization Bill
Senate Health Committee Passes Prior Authorization Bill
The Senate Committee on Health and Provider Services unanimously passed Senate Bill (SB) 3 on Wednesday. This bill, authored by Sen. Tyler Johnson (R- Leo), would place limitations on how health insurance providers use prior authorization in certain circumstances when making coverage decisions.
IHA strongly supports this legislation and appreciates Senate leadership prioritizing a bill which would streamline the process to allow physicians to spend more time seeing patients, and less jumping through unnecessary hoops. This bill would significantly improve the system, putting the patient first.
Dr. Elizabeth Wright, Chief Ambulatory Officer at Hendricks Regional Health, testified in support of the bill, saying patients deserve, and expect health coverage that does not interfere with care they discuss and decide upon with their physician. SB 3 prioritizes and protects the patient-physician relationship which is crucial to ensure the most appropriate care is delivered.
 Hospitals Still Need Your Help
Hospitals Still Need Your Help
Thank you for your advocacy on behalf of your hospital over the last week.
IHA’s top priority for the 2024 session is HB 1393 which is the first step in modernizing Indiana’s Medicaid system, specifically looking at the Hospital Assessment Fee (HAF) program and establishing a Managed Care Assessment Fee (MCAF).
Beacon Health System CEO Kreg Gruber, IU Health CEO Dennis Murphy, Deaconess Hospital CEO Shawn McCoy, and Union Health CEO Steve Holman joined the IHA advocacy team to meet with Speaker Todd Huston and the Governor’s office to continue education on HB 1393 and the urgent need to help our hospitals.
The IHA advocacy team will continue to meet with legislators to discuss the importance of this bill, but we still need your help. Please reach out to your representatives and senators, asking them to vote “yes” on this bill. Please click the button below to send a pre-written message directly to the legislators who represent your district. Estimated time 2-3 minutes.
Click the button below to send a pre-written message directly to the legislators who represent your district. Estimated time 2-3 minutes.
Here's how it works:
-
Click the red button below to open the IHA Action Center.
-
Once open, there will be a sample message drafted in the Message Body section —feel free to customize this message to reflect your individual hospital.
-
Next, fill out your contact info in the boxes below the Message Body section.
-
Once complete, hit the blue “send message" button to ensure your voice is heard. You will receive a confirmation email notifying you that your message was successfully sent and to which legislators. Note: First-time users will need to authenticate by verifying their email. Be sure to check your junk/spam if you do not see that message.
 IHA Opposes Bill That Leads to More Cost Shifts
IHA Opposes Bill That Leads to More Cost Shifts
HB 1200 would arbitrarily set caps on reimbursement that would not take into account the payor mix and cost pressures, or the level of services being provided to state employees at each individual hospital. This bill would result in further cost-shifting to all other employers in the state.
Mike Schroyer, CEO of Baptist Health Floyd, testified on behalf of IHA in opposition to the bill and said to, “Instead of pursuing price caps, which were debated and not pursued just last year by this body, we would encourage the legislature to work with the State Personnel Department to learn more about their tiered network program HealthSync, was launched just a few years ago to incentive state employees to schedule with preferred providers with lower visit costs through lower deductibles and lower out-of-pocket maximums.”
Shroyer continued to say incentivizing low-cost providers through a tiered network system is the right, pro-market approach for Indiana, and if further updates to that program would maximize the benefit, hospitals would welcome that discussion – but price caps are not the answer.
The bill was held by the Committee on Insurance, and IHA will continue working with legislators on a viable plan to reduce cost shift rather than a measure that would squeeze the proverbial balloon of health care costs. The bill will continue to be considered by the committee and IHA will update members on its status through the legislative process.
Legislative Update - January 12, 2024
 Governor Holcomb Releases 2024 Next Level Agenda
Governor Holcomb Releases 2024 Next Level Agenda
The 2024 legislative session kicked off with Gov. Holcomb announcing his 2024 Next Level Agenda for his final year as Indiana Governor. The agenda includes priorities for the legislative session and the implementation of other initiatives in state government. His health agenda items are as follows: The Holcomb administration's agenda includes prioritizing K-12 and higher education, making childcare more affordable, strengthening Indiana's economic outlook, additional workforce development measures, and improving services for aging Hoosiers.
For more information on Gov. Holcomb's 2024 Next Level, click
here.
IHA 2024 Legislative Agenda
IHA's top priority for the 2024 session is
HB 1393 which is the first step in modernizing Indiana's Medicaid system, specifically looking at the Hospital Assessment Fee (HAF) program and establishing a Managed Care Assessment Fee (MCAF). IHA's proposal for the upcoming session is to update the HAF program to allow hospitals to be assessed up to the federally allowable maximum to increase the overall benefit of the HAF program and protect access to quality care across the state. In addition to protecting access, our proposal will help reduce the cost shift to commercial insurance. We look forward to partnering with policymakers to protect access to care at no cost to the state under this proposal while helping to reduce the cost shift paid for by employers and consumers.
ACT NOW: Please reach out to your lawmakers this week and ask them to vote yes on
HB 1393. We have drafted a pre-written message to send to your legislators that can be customized to share what specific issues your hospital is facing.
Click the button below to send a pre-written message directly to the legislators who represent your district. Estimated time 2-3 minutes.
Here's how it works:
-
Click the red button below to open the
IHA Action Center.
-
Once open, there will be a sample message drafted in the Message Body section —feel free to customize this message to reflect your individual hospital.
-
Next, fill out your contact info in the boxes below the Message Body section.
-
Once complete, hit the blue “send message" button to ensure your voice is heard. You will receive a confirmation email notifying you that your message was successfully sent and to which legislators.
Note:
First-time users will need to authenticate by verifying their email. Be sure to check your junk/spam if you do not see that message.
 Indiana General Assembly Announces Agenda
Indiana General Assembly Announces Agenda
The Indiana Senate and House released their agenda bills for the 2024 Legislative Session.
The Senate Republicans' agenda focused on improving Hoosier students' reading skills, childcare access, protecting patients, fiscal responsibility, government accountability, and upgrading water lines to protect Hoosiers' health.
The Senate and House Democrats released a joint agenda they hope to tackle this session. The agenda focused on increasing access to affordable, high-quality childcare, providing all homeowners with property tax relief, capping prescription drug costs, solving the third-grade reading proficiency crisis, and creating citizen-led ballot referendums.
The
House Republicans released their agenda
which focuses on five key parts: Expanding work-placed learning, “stepping up" for retirees, boosting student reading proficiency, protecting taxpayers, and supporting Jewish students in Indiana.

Legislative Update - November 17, 2023

Health Care Cost Oversight Task Force Issues Recommendations
On Nov. 13, the Health Care Cost Oversight Task Force concluded it final meeting of 2023, issuing recommendations for the first year of the two-year task force.
As a part of the final meeting, Nate Kauffman provided a presentation on the impact of prior authorization on physician burnout, hospital costs, and adverse events for patients. Mr. Kauffman noted Indiana has one of the highest denial rates in the nation at 23.6%. Mr. Kauffman recommended that significant cost savings could be achieved if insurance administrative processes were standardized rather than being unique for each company, and if one neutral third party was responsible for determining medical necessity for all payers. Mr. Kauffman also recommended the task force consider legislation to promote transparency and penalize payers for inappropriate denials and delays in payment.
The task force then went on to adopt a Final Report, and the task force’s recommendation regarding prior authorization was notably strengthened following Mr. Kauffman’s presentation. Through its Final Report, the Task Force recommends:
-
Specifying that employers have full ownership and control over health claims data related to their covered lives.
-
Maintaining that employers can audit health claims and provider payments but third-party administrators, insurers, or pharmacy benefits managers (PBMs) shall not charge a fee for such an audit.
-
Prohibiting spread pricing by PBMs, where a managed care organization is charged more for a drug than what the PBM pays a pharmacy.
-
Requiring health care entities seeking to merge and acquire another entity to provide notice to legislative leadership. The recommendation noted that the General Assembly should consider applying this notice requirement only to companies above a certain revenue or market share.
-
Increasing transparency for prior authorizations and denials. Specifically, examining ways to standardize the process, establishing a penalty for inappropriate denials or delays, and requiring insurers to provide explanations for those denials.
-
Requiring PBMs, third-party administrators, employee benefits consultants, and insurance brokers to act as fiduciaries.
-
Establishing a report for Indiana’s physician reimbursement rates and professional services fees for the commercial market compared to a statewide average benchmark.
IHA was encouraged by many of the recommendations but will work with legislative leaders to learn more about the merger and acquisition recommendation and reporting physician reimbursement rates to ensure overburdensome regulations do not continue to be enacted on Indiana’s health care entities.
 Land Use Task Force
Land Use Task Force
The Land Use Task Force also issued its Final Report and recommendations this week on Nov. 14, which included improving access to medical services in rural and blighted communities, including OB-GYN services, trauma centers, and general health services, to help remove barriers to community growth. Brenda Reetz, CEO of Greene County Community Hospital, previously testified on Oct. 20 to support this recommendation, including recommending the legislature enact changes to the hospital assessment fee statute to increase Medicaid reimbursement for Indiana’s hospitals.
 Medicaid Oversight Committee
Medicaid Oversight Committee
Finally, the Medicaid Oversight Committee met on Nov. 15 to learn more about Indiana’s recent growth in Medicaid expenditures. The committee heard presentations on various topics, including the most & least utilized services in managed care programs, and Indiana Medicaid mandatory and optional services. The committee concluded its last meeting of 2023 and does not intend to issue any recommendations until next year.
IHA’s Government Relations Team will continue to keep you updated as the 2024 legislative session approaches in January.
Legislative Update - June 16, 2023
 Legislative Study Committee Topics Assigned
Legislative Study Committee Topics Assigned
Each year after the legislature adjourns, the Legislative Council will convene to formally assign topics for interim study committees to review before the next session. The council is comprised of leaders from each of the four caucuses, and they choose subjects based on directives included in recently enacted legislation and requests submitted to council members by other members of the general assembly. Study committees will meet over the next several months to review such assigned topics and issue a public report on its findings and any recommendations the committee approves. Below are the topics set by the legislative council that are relevant to the health care industry. You will see topics assigned that were included in Senate Enrolled Act (SEA) 400, a priority bill for IHA. Our advocacy team will continue providing updates on these items as their respective committees review them.
Study Committee on Employment and Labor:
-
Whether Indiana should adopt interstate mobility of occupational licensing to allow individuals who hold current and valid occupational licenses or government certifications in another state in a lawful occupation with a similar scope of practice as Indiana to practice in Indiana under certain conditions. (Source: SEA 400 (2023)
Study Committee on Financial Institutions and Insurance:
-
Whether a health insurer or a health maintenance organization should be required to exempt a participating health care provider from needing prior authorization on a particular health care service if the participating health care provider has continuously received approval for the health care service for a determined number of months. (Source: SEA 400 (2023))
Study Committee on Public Health, Behavioral Health, and Human Services:
-
Options for child care, including the location of childcare facilities in businesses or other commercial buildings. (Source: Letter, Sen. Brown, Sen. Taylor, Rep. Lehman)
The following topics:
-
The prevalence and impact of mental illness, including major depression disorder, post-traumatic stress disorder, and severe anxiety, among veterans and first responders in Indiana.
-
Alternative treatment options for severe mental illness that have been given "breakthrough therapy" status by the United States Food and Drug Administration, including psilocybin for treatment-resistant depression.
-
Policies enacted and under consideration in other states that enable access to psilocybin-assisted therapy for veterans, first responders, and others experiencing severe mental illness. (Source: Letter, Rep. Teshka, Rep. Bauer, Rep. Willburn, and others).
Health Care Cost Oversight Task Force:
-
Oversight of health care costs (Source: HEA 1004 (2023))
Medicaid Oversight Committee:
-
Review, consider, and make recommendations concerning all requests for new services and changes in existing services for the Medicaid program. (Source: IC 12-15-47.3; HEA 1001, SECTION 137 (2023))
 Lt. Gov. Visits Greene County General Hospital
Lt. Gov. Visits Greene County General Hospital
Lieutenant Governor Suzanne Crouch traveled around the Wabash Valley earlier this week and stopped in Linton to visit with the team at Greene County General Hospital. CEO Brenda Reetz said the visit was productive, and the Lieutenant Governor was able to see firsthand convenient, quality care delivered by the hospital despite the significant challenges they are facing. Crouch, who is running for Governor in 2024, says lawmakers have focused on health care recently, but there is still work to be done.
"While the General Assembly focused on hospitals this past session, hospitals alone are not responsible for rising health care costs and, so, we, as a state, need to take a holistic look at the problem and find a solution where everybody has a little give and take that results in quality health care but affordability for Hoosiers," Crouch said. IHA agrees that a comprehensive approach should be taken to improving health care for Hoosiers, and that includes all stakeholders in the industry that contribute to the costs paid by businesses and individuals. We look forward to continuing our advocacy for such an approach. Above are photos from Greene County General Hospital Facebook page. You can also read the local news
story covering the visit.
 PBMs Remain Target in D.C.
PBMs Remain Target in D.C.
Earlier this week Chairman of the U.S. Senate Finance Committee Senator Ron Wyden (D-OR), along with others, introduced the Patients Before Middlemen (PBM) Act to delink the compensation of pharmacy benefit managers (PBMs) from drug price and utilization to align better incentives that will help lower prescription drugs costs for Medicare Part D beneficiaries. Chairman Wyden stated, "This legislation will put a stop to one of the most egregious practices driving up the price of prescription drugs in Medicare: pharmacy benefit managers getting paid based on the price of a drug . . . Instead of fighting for lower prices, this practice has encouraged drug middlemen to favor higher-priced drugs in their negotiations, which means seniors are forced to pay more for their prescriptions."
Ranking member of the committee, Senator Mike Crapo (R-ID), added, "As we work to find solutions that reduce prescription drug costs for patients at the pharmacy counter, this commonsense proposal will help mitigate misaligned incentives that currently steer some Medicare Part D plans, pharmacy benefit managers and seniors toward higher-priced medications, even when more affordable alternatives like biosimilars are on the market . . . Delinking PBM compensation from sticker prices would take a critical first step in ensuring that all supply chain participants seek out the best deals available, driving down out-of-pocket spending and promoting cost-cutting competition."
The PBM Act would:
-
Prohibit PBM compensation based on the price of a drug as a condition of entering into a contract with a Medicare Part D plan. Service fees will not be connected to the price of a drug, discounts, rebates, or other fees.
-
Create an enforcement mechanism requiring PBMs to pay the Secretary any amount over the designated service fees.
We see that the current system incentivizes PBMs to steer health plans and seniors toward more expensive prescription drugs, which runs counter to the industry's goal when it was created – help employers manage prescription drug costs. Indiana's lawmakers have examined the industry in recent years, and in 2020 began requiring them to register with the Indiana Department of Insurance (IDOI) for oversight and enforcement of unfair practice violations. We believe there will be continued interest in regulating this industry and look forward to assisting policymakers in striking the right balance in future sessions.
Read the PBM Act.
Legislative Update - June 2, 2023

IHA Priority Bill Signed
Surrounded by key stakeholders and the legislators who worked on the legislation, Governor Eric Holcomb ceremoniously signed Senate Enrolled Act (SEA) 400. This legislation was one of the most impactful health care bills of the 2023 legislative session and a top priority for the Indiana Hospital Association. SEA 400 increases transparency in the review process for insurer premium increases, streamlines provider credentialing, and improves the prior authorization process for providers and patients. Julie Slinker, Senior Director of Revenue Cycle for Rush Memorial Hospital, and Trent Fox, IHA Vice President of Government Relations, attended the ceremony. Julie played a crucial role in the passage of this bill by helping IHA craft this measure and educating lawmakers on its importance by testifying in support of the bill.
Learn more about SEA 400.

Technical Corrections Day Canceled
The Indiana General Assembly's "Technical Corrections Day" has been canceled by a joint order from Speaker of the House Todd Huston and President Pro Tempore of the Senate Rodric Bray. The legislature schedules a day every year post-session for necessary technical corrections resulting from all the newly passed laws. The changes made on such days are only needed to ensure law consistency and avoid conflicting language. Therefore, substantive changes are not permitted.
For example, statutes that include cross-reference citations to other areas of law could contain outdated citations depending on what legislation was passed. Therefore, such a technical correction would be necessary to ensure accuracy in applying state law.
Read the joint order.

Health Care Issues on the Hill
Federal lawmakers have been busy with several issues lately, the most popular right now being the debt ceiling negotiations. However, they are also considering legislation that would significantly impact the health care industry, specifically hospitals. The two issues moving through the process now that need your attention are "site-neutral" cuts and burdensome 340B reporting. The "site-neutral" included in
H.R. 3561 proposal will negatively impact reimbursement by requiring each off-campus outpatient department of a provider to obtain and provide a national provider identifier on billings for claims for services and requiring drug administration services furnished in off-campus provider-based departments (PBDs) to be paid at a site-neutral rate, which is estimated to result in a cut to hospitals of $54.2 million in the first year and $3 billion over ten years.
Read the entire bill or the
U.S. House Energy and Commerce Committee's summary.
The proposal regarding the 340B Drug Pricing Plan is being marketed as increased transparency, a concept IHA embraces. However, the reporting requirements in the current legislation are simply over burdensome and will not provide policymakers with meaningful information.
Read the current version of the bill.
Lastly, the U.S. Senate Finance Committee will hold a hearing next week to discuss the agenda topic "Consolidation and Corporate Ownership in Health Care: Trends and Impacts on Access, Quality, and Costs."
Learn more about the committee and watch the hearings.
In coordination with member hospitals, IHA's advocacy team continues to monitor and provide input to Indiana's congressional delegation.
End of Session Update - Legislative Update - May 19, 2023

Priority Mental Health Bills Signed into Law
Earlier this week at the Indiana Mental Health Summit, Governor Eric Holcomb ceremoniously signed Senate Enrolled Act (SEA) 1 and House Enrolled Act (HEA) 1006. Several key stakeholders were in attendance, including Goerge Hurd, Vice President of Community Fairbanks Behavioral Health. Both bills are significant steps in the right direction to address the needs of the state. SEA 1 is a priority for both the Governor and the General Assembly and includes funding in the state budget in the amount of $100M over the biennium. The new law allows a state plan amendment or waiver to require reimbursement for eligible certified community behavioral health clinics and reestablishes the Indiana Behavioral Health Commission. HEA 1006 streamlines the immediate detention process and provides liability protections for facilities, law enforcement, and practitioners. Under the combined process, an individual may be detained at a facility for 72 hours from the time of admission, with certain exclusions, including weekends and legal holidays. The law also states that services provided under this process shall be deemed medically necessary for reimbursement.

IHA Legislative Summary
As a follow-up to our last legislative update covering various legislation passed during the 2023 session, IHA Deputy General Counsel Laura Brown compiled a memorandum outlining each House Enrolled Act (HEA), and Senate Enrolled Act (SEA) passed during the Indiana General Assembly's 2023 legislative session impacting IHA members. IHA will also be distributing more specific guidance on the hospital fiscal reporting language contained in HEA 1004 and the medical error reporting language contained in SEA 400 next week. IHA is working with members of the Council on Finance to develop the hospital fiscal reporting guidance. You can find the memo here. Additionally, please join Hall Render's Kevin Stella and Dana Stutzman, and IHA's Laura Brown for a webinar on the impact of SEA 7 on May 23rd at 1 PM ET. To learn more and register, please click
here.

The Legislative B-Side
During each session, many bills receive significant attention, and the focus typically falls on the proposals moving forward through the process. What doesn't make headlines are the items that are defeated before crossing the finish line, and often those are considerable victories on their own. We are extremely proud of the work IHA's advocacy team completed concerning proactive measures, but we want to take this opportunity to highlight several harmful or unnecessary items that were neutralized or defeated by the team.
Harmful proposals that IHA neutralized and/or killed:
- HB 1271: Additional public forum requirements (reporting, notice, etc.)
- HB 1291: Burdensome reporting of 340B, hospital MLR, and CARES Act funding
- SB 288: Concerning wrongful death proposal (medical malpractice statute implications)
- HB 1075: Expanded civil investigative demand authority for AG over non-profit hospitals
- HB 1454: Increased property taxes for investor-owned hospitals
- HB 1462: Burdensome ED reporting re SUD plans
- HB 1003: Intrusive contract interference limiting deviation from previous insurance contracts
- HB 1212: Unnecessary disclosure requirements for hospital foundations
- HB 1179: Inconsistent and antiquated licensing board meeting proposal
- HB 1001: Increased HAF burdens to fund other Medicaid priorities
Legislative Update - April 28, 2023
 2023 Legislation Session Complete
2023 Legislation Session Complete
The 2023 legislative session ended very early this morning, around 2:30 a.m. Lawmakers packed several significant developments into the final day of session, including school funding formulas, local government finance, and health care costs. As you know, we have been advocating for a responsible way for the state to govern health care costs – incentivize market solutions and create a framework for equal accountability for all stakeholders, especially insurance companies.
Unfortunately, the legislature mainly focused on hospitals in their proposals and did without adequate assistance to address Indiana's low Medicaid rates that haven't been updated in over twenty years. IHA's members will continue their commitment to affordability and keep advocating for less government interference which only hinders such efforts. Please see the statement from IHA President Brian Tabor on the passage of the budget and HB 1004. Additionally, IHA will be sending out a more comprehensive update on legislation impacting members in the coming weeks.
 HB 1001: The State's Biennial Budget
HB 1001: The State's Biennial Budget
The number one priority for lawmakers this session was HB 1001, the state's biennial budget, and it passed in its final form mainly along a party-line vote in both the House and Senate. The budget funds the Medicaid forecast increases Medicaid physician reimbursement up to Medicare levels, funds the Governor's Public Health Commission recommendations at $75 million for State Fiscal Year (SFY) 2024, and $150 million for SFY 2025, provides $100 million for community mental health centers over the biennium, and allocates $10 million in SFY 2024 for regional mental health facility grants. In addition, it includes language to require the Office of Medicaid Policy & Planning to conduct a rolling Medicaid rate review every four years.
 HB 1004: Hospital Price Targets and Site of Service
HB 1004: Hospital Price Targets and Site of Service
During the final hours of session,
HB 1004, the legislature's priority health care bill, was agreed upon between the House and Senate and now heads to the Governor for his signature.
In its final version, HB 1004 requires the Indiana Department of Insurance to measure hospital prices against the target, which the legislation determined to be 285% of Medicare. The calculation of each health system's prices includes inpatient, outpatient, and physician prices. Under the site of service language, such hospitals would not be able to assess a facility fee for office settings 250 feet away from the hospital's main building. Oncology treatment centers and behavioral health services were exempted from the prohibition and office settings where invasive procedures are provided based on the definition of "office setting." The price targets and site of service provisions apply to hospital systems with an annual patient service revenue of at least $2 billion, based on the hospital system's 2021 audited financial statement.
The bill also requires all hospitals to include additional information in their yearly fiscal reports with the Indiana Department of Health, including net patient revenue for outpatient, inpatient, and professional services. In addition, under the bill, third-party administrators would be required to provide claims data to plan holders within 14 calendar days of a request.
 IHA Agenda: 3 for 3
IHA Agenda: 3 for 3
All three of IHA's legislative agenda bills have been approved by final votes and are on their way to the Governor's desk for a final signature. HB 1460 modernizes and streamlines the Indiana Professional Licensing Agency's (PLA) licensing process.
HB 1021 now includes increased penalties for violence against all emergency room staff. SB 400 improves insurance transparency and provider credentialing. The bill created a pilot program with the state employee health plan for prior authorization relief, received overwhelming support, and will become law in the coming days.
Legislative Update - April 21, 2023
 HB 1004 Amended on 2nd Reading
HB 1004 Amended on 2nd Reading
On Apr. 17, the Senate amended HB 1004 on 2nd Reading to remove the requirement that nonprofit hospital systems meet 260% of Medicare for hospital facility prices or otherwise be assessed a penalty. In its place, site of service language was added for hospital systems with an annual patient service revenue of at least $2 billion, based on the hospital system's 2021 audited financial statement. Under the site of service language, such hospitals would not be able to assess a facility fee for office settings 250 feet away from the hospital's main building. Oncology treatment centers and behavioral health services were exempted from the prohibition and office settings where invasive procedures are provided based on the definition of "office setting."
The bill also requires all hospitals to include additional information in their yearly fiscal reports with the Indiana Department of Health, including net patient revenue for outpatient, inpatient, and professional services. In addition, under the bill, third-party administrators would be required to provide claims data to plan holders within 14 calendar days of a request.
As amended, HB 1004 passed the Senate on 3rd Reading on Apr. 18. The House has since dissented on the Senate changes, sending the proposal to conference committee where a final version will be negotiated and presented to both bodies for final adoption. IHA's legislative team will continue discussions with legislative leaders as the final proposal is discussed.
 Medicaid and Revenue Forecasts Released
Medicaid and Revenue Forecasts Released
In anticipation of the final version of the state's biennial budget being released next week, the State Budget Committee heard updated Medicaid and revenue forecasts this week to consider as the final budget proposal is crafted.
The full Medicaid forecast can be found
here. Under the updated revenue forecast, which was initially released in December 2022, Indiana is expected to collect $1.5 billion more in revenue than originally anticipated over the next two state fiscal years. Fiscal years in Indiana begin on July 1 and end on June 30 of the following year.
 Looking Ahead
Looking Ahead
The 2023 legislative session must adjourn by Apr. 29, and IHA expects its legislative agenda bills to be finalized throughout next week. IHA will keep you updated in the remaining days and issue a comprehensive overview of each health care bill enacted the week following the legislative session's conclusion.
Legislative Update - April 14, 2023
 IHA Priority Bills One Step Closer to Law
IHA Priority Bills One Step Closer to Law
This week, all three of IHA’s legislative agenda bills advanced to bring them one step closer to becoming law. HB 1460, one of IHA’s agenda bills, modernizing and streamlining the Indiana Professional Licensing Agency’s (PLA) licensing process, was passed by the Senate unanimously and returns to the House where we expect a concurrence and final passage. SB 343, which now includes increased penalties for violence against all emergency room staff, was passed by the House by a vote of 85 to 12 and now returns to the Senate for either a concurrence or dissent. SB 400, IHA’s priority bill regarding insurance transparency and provider credentialing, passed the House unanimously and returns to the Senate, where we expect a dissent in order to address one provision’s fiscal impact. This bill has had significant support throughout the process,therefore we are confident it will be passed into law soon.
 Problematic Bills Advance
Problematic Bills Advance
HB 1004, which caps hospital prices at 260% of Medicare and includes steep penalties, was passed out of the Senate Appropriations Committee. The bill will now be considered by the full Senate. The penalties on nonprofit hospital systems have been expanded to create an arbitrary cap based on the 260% percentage of Medicare. The IHA team continues to engage legislative leadership and anticipates changes on second reading next Monday. Another concerning bill significantly restricting the ability to enforce non-competes, SB 7, was amended in the House Employment Committee this week after failing to pass in the same committee last week. The bill will be considered by the full House next Monday for a final vote.
 Senate Budget Released
Senate Budget Released
On Apr. 13, the Senate Appropriations Committee released the Senate’s version of the state’s biennial budget, HB 1001. The current proposal fully funds the Medicaid forecast at $7.5 billion over the biennium (a $2 billion biennial increase), funds the Governor’s Public Health Commission recommendations at $75 million for State Fiscal Year (SFY) 2024, and $150 million for SFY 2025, provides $35 million for community mental health centers over the biennium, and allocates $10 million in SFY 2024 for regional mental health facility grants. HB 1001 also continues to fund Medicaid physician reimbursement at 90% of Medicare. It includes language to require the Office of Medicaid Policy & Planning to conduct a rolling Medicaid rate review every 4 years.
HB 1001 passed out of the Senate Committee by a vote of 10-2 and now heads to the full Senate for consideration. IHA continues to discuss Medicaid assistance for all hospitals with legislative leadership for inclusion in the final version of the budget, which will be released prior to Apr. 29.
Legislative Update - April 7, 2023
 IHA Workforce Agenda Bill Advances
IHA Workforce Agenda Bill Advances
On Wednesday, Apr. 5, the Senate Health & Provider Service Committee heard HB 1460, one of IHA’s agenda bills, modernizing and streamlining the Indiana Professional Licensing Agency’s (PLA) licensing process. Rachel Culpepper, the General Medicine Service Line Director for IU Health West, testified in support of the bill, which passed by a vote of 10-0.
Highlights of the bill are as follows:
-
The bill allows PLA licensing boards to meet virtually to remove barriers for the boards to convene to review and approve licenses.
-
The bill allows PLA to standardize the form of applications across all boards to ease processing.
-
The bill requires PLA to send notification of incomplete items in an application to an applicant every 14 calendar days until the application is completed.
-
The bill requires full reciprocal licenses to be issued within 30 days.
-
The bill requires PLA to post board agendas, minutes, and board vacancies within specific timeframes to ensure all stakeholders have timely access to that information.
-
The bill requires all applications to be submitted electronically unless a paper copy is requested from PLA, as many times paper applications cause processing delays.
-
The bill creates a temporary nurse permit to allow nurse applicants to practice until an applicant’s NCLEx results are received.
HB 1460 now moves to the entire Senate floor for a vote.
 Senate Committee Passes Unprecedented Caps
Senate Committee Passes Unprecedented Caps
The Senate Health & Provider Services Committee also amended HB 1004 onWednesday, taking a step in the wrong direction on the legislation.
The penalties on nonprofit hospital systems have been expanded to create an arbitrary cap based on the 260% percentage of Medicare. Meanwhile, language requiring accountability for insurance companies added in the House of Representatives was deleted. As amended, the bill passed by a vote of 6-5 and was recommitted to the Senate Appropriations Committee.
Read IHA's public statement on the proposal.
The IHA team continues to engage legislative leadership and anticipates changes in the Senate Committee on Appropriations.
 Noncompete Ban Stalls
Noncompete Ban Stalls
On Thursday, Apr. 6, the House Employment, Labor, and Pensions Committee heard SB 7, which, as it passed the Senate, would prohibit an employer and physician from entering into a new noncompete agreement after July 1, 2023. Dr. David Dunkle, CEO of Johnson Memorial Health, testified to outline IHA’s concerns with eliminating noncompete agreements as a legitimate business tool.
The House Committee amended the bill to narrow the language that will only prohibit noncompete agreements for primary care physicians. Still, as amended, the bill failed to move forward by a vote of 6-6.
Since the bill was not decisively defeated, the bill is still eligible for another hearing next week. IHA’s team will continue to engage on this critical issue and keep you updated.
Thank you to all of IHA’s members who testified on bills this week and continue to engage legislators on matters impacting hospitals.
Legislative Update - March 31, 2023
 IHA Priority Bill Continues to Move
IHA Priority Bill Continues to Move
SB 400, one of IHA's priority bills regarding insurance transparency and provider credentialing, passed out of House Health Committee on Monday and was reassigned to House Ways & Means Committee. Julie Slinker, Senior Director of Revenue Cycle at Rush Memorial Hospital, testified in support of the bill on behalf of IHA and did a fantastic job explaining the importance of the provisions in the legislation. The bill has been amended throughout this process, as expected, and contains significant improvements to the laws governing provider credentialing to ensure no unnecessary delays in the future. Additionally, it establishes a pilot program that eliminates the requirement of prior authorization for commonly approved CPT codes for the state employee health plan.
Upon completion of the pilot program, policymakers will review the results and outcomes to determine what next steps should be implemented to improve the prior authorization framework.
The bill also includes improvements to the rate review process IDOI utilizes when approving insurance premium increases. The bill passed the Senate 48-0, and we expect the bill to reach the Governor's desk in the coming weeks.
 Health Care Workers' Protections are now "Safe and Sound" After Passing Committee
Health Care Workers' Protections are now "Safe and Sound" After Passing Committee
On Wednesday, IHA Board member Larry Tracy, President of Memorial Hospital of South Bend, testified in support of adding language to SB 343 to increase penalties for violence against all emergency room staff. The amendment was successfully added, and we want to thank IHA's advocacy team for their persistence. Even though the bill we supported was not heard in the first half of session, they didn't give up, and we now have a chance to enact this third priority. Please also remember that legislation is only one component of IHA's Board-led "Safe and Sound" initiative to improve workforce safety. IHA's patient safety team is now rolling out the
"Safe & Sound" communication toolkit across our membership, working with your teams. Additionally,
a recent news story covered the "Safe & Sound" campaign. We thank 2022 Chair Brad Smith for creating this initiative and for Larry's strong support as the Council on Quality and Patient Safety Chair.
 Price Controls Debated By Senate Committee
Price Controls Debated By Senate Committee
HB 1004 was heard in the Senate on Wednesday, but there needed to be a consensus on how to proceed (read the news story). A positive development was much discussion of increasing Medicaid rates and addressing low physician reimbursement. IHA Chair Carol Dozier, and IHA President Brian Tabor superbly represented hospitals.
Watch the hearing by selecting "Wednesday, Mar 29 - 9:00 am". The bill, as currently drafted, establishes a health care cost control board to collect and analyze data and directs the Indiana Department of Insurance to establish a national average related to pricing, which hospitals will be required to achieve within a specific timeframe. The committee chair held this bill. It will be amended next Wednesday before moving to the next phase in the process, which is likely to be a recommitment to the Senate Appropriations Committee, where the bill's fiscal impact will be reviewed. IHA has been working tirelessly to ensure lawmakers at every level understand the effect of this legislation and continue to offer solutions to improve it.
Legislative Update - March 24, 2023
Emergency Detention Streamlining

On Mar. 21, the Senate Corrections and Criminal Law Committee heard
HB 1006, which streamlines the immediate and emergency detention statutes into the emergency detention statute.
Under the proposal, an emergency detention application must be filed within 48 hours, and then the individual may continue to be held for 72 hours while a court determines probable cause. Emergency services may be provided during this time, and upon the finding of probable cause, a court may order treatment in accordance with a mental health or substance use disorder treatment plan using accepted clinical care guidelines, including medication, pending a final hearing.
Importantly, the bill provides that services provided to an individual subject to emergency detention are medically necessary for purposes of Medicaid reimbursement and commercial insurance. The bill also provides liability protections for an act or omission taken in good faith under the emergency detention law for facilities, law enforcement officers, superintendents, physicians, advanced practice registered nurses, and physician assistants.
The bill passed by a vote of 7-1 and was reassigned to the Senate Appropriations Committee, where it is expected to receive a hearing in the coming weeks.
Prescription Drug Rebates

On Mar. 22, the House Insurance Committee heard
SB 8, which would require, for individual health insurance coverage, the defined cost sharing for a prescription drug to be calculated at the point of sale. For group health insurance coverage, an insurer would be required to pass through to the plan sponsor 100% of all rebates received or estimated to be received by the insurer concerning the dispensing or administration of prescription drugs to the covered individuals of the plan sponsor.
A Committee Amendment was offered on the bill that would require pharmacies to include a modifier for 340B drugs that are dispensed, but the bill was held for further consideration next week. IHA’s legislative team will continue to monitor the bill and engage legislators on the impact of the proposed modifier amendment.
PBM Rule Finalized

On Mar. 22, the Indiana Department of Insurance (IDOI) published a
final rule concerning pharmacy benefit managers (PBM) to set forth provisions for PBM licensure, pharmacy claims audits, maximum allowable cost pricing, annual reporting, and penalties for violations. The final rule is effective 30 days from its publication.
Going forward, PBMs will be required to obtain a license from IDOI and include a current audited annual financial statement in their license application. The license is valid for a one (1) year period and must be renewed thereafter.
Under the final rule, a PBM may cause an audit to occur at a particular pharmacy location not more than one (1) time per calendar year. However, if the audit results in a finding of material noncompliance at the pharmacy, the auditor may return within the calendar year to determine ongoing compliance. The final rule then goes on to outline parameters for audits, including:
• Prohibiting audits from occurring during the first seven (7) calendar days of a month without the voluntary consent of the pharmacy;
• Prohibiting payments to an auditor based on a percentage of the amount recovered as a result of an audit; and
• Requiring auditors to allow pharmacies to produce documentation to address a discrepancy found during an audit. Specifically, if a clerical error is identified during the course of an audit, the pharmacy must be allowed to obtain a prescription that corrects the clerical error from the prescriber.
The final rule also specifies that an audit finding of an overpayment or underpayment of a claim must be based on an actual overpayment or underpayment of the audited claims, and not an extrapolation.
Finally, regarding maximum allowable cost pricing, PBMs will be required to update their maximum allowable cost list at least every seven (7) calendar days, and a pharmacy must be given the right to obtain a current list of the sources used by the PBM to determine maximum allowable cost pricing within ten (10) calendar days of a request. Further, in order to place a prescription drug on a maximum allowable cost list, a PBM must ensure that the drug is generally available and listed as "A" or "B" rated in the most recent version of the United States Food and Drug Administration's Approved Drug Products with Therapeutic Equivalence Evaluations.
Legislative Update - March 17, 2023
Governor's Public Health Bill Received Input
The House Public Health Committee heard testimony on
Senate Bill (SB) 4 on Tuesday morning and will likely be scheduled for amendment and committee vote next week. The bill, which is part of the Senate Republican Legislative Agenda and a priority for Governor Holcomb, has resulted in various reactions through the legislative process. SB 4 is the legislative recommendation from the Governor's Public Health Commission, established to address the lessons learned through the COVID pandemic.
SB 4 results from the recommendations given by the Governor's Public Health Commission, which was created to assess and improve Indiana's public health infrastructure. IHA President Brian Tabor and other leaders in Indiana's health care community participated in the commission to make the recommendations. Currently, the funding for this initiative is located in the state budget bill, HB 1001, where the proposed funding is $75M for the first year and $150M for the second year of the biennium.
You can read the full text of the bill here.
 Priority Bill Passes out of Committee
Priority Bill Passes out of Committee
The Senate Committee on Insurance and Financial Institutions voted to send
House Bill (HB) 1003 to the full Senate earlier this week. HB 1003 consists of two major components: (1) tax credits for non-traditional health reimbursement arrangements; and (2) encouragement of value-based contracting between insurers and providers.
The bill, which is part of the House Republican Caucus legislative agenda, has improved significantly since it was introduced. There was some extremely harmful and intrusive interference with contracts that were fortunately amended from the bill. Currently, the bill allows a credit against the state tax liability of an employer with fewer than 50 employees if the employer has adopted a health reimbursement arrangement instead of a traditional employer-provided health insurance plan. Additionally, it provides that a health care provider that enters into a value-based health care reimbursement agreement with a health plan may qualify to participate in the health plan's program to reduce or eliminate prior authorization requirements.
The concepts in this bill are generally positive, but IHA has advocated ensuring they remain optional to avoid reducing flexibility in negotiations tailored to each community's needs. You can read the full text of the bill here.
 IHA Submits Comments on Proposed PA Rule
IHA Submits Comments on Proposed PA Rule
IHA has submitted comments to CMS regarding its proposed rule to improve prior authorization under Medicare Advantage, Medicaid and CHIP state agencies, Medicaid managed care plans, CHIP managed care plans, and qualified health plan issuers. A summary of the proposed rule can be found here.
In submitting its comments, IHA urged CMS to finalize the proposed rule with the inclusive plans and to move forward with requiring impacted payors to provide a specific reason for prior authorization denials.
Concerning reducing prior authorization timelines, IHA recommended that plans be required to deliver prior authorization responses within 72 hours for standard, non-urgent services and within 24 hours for urgent services, rather than 72 hours and seven (7) calendar days, respectfully. IHA also urged that the plans be required to report metrics on their prior authorization processes and recommended that CMS regularly audit a sample of plan denials and timeframes.
On any interoperable electronic prior authorization processes, it is critical that any solution be fully developed and tested before wide-scale industry rollout and required usage. IHA will continue to monitor the proposed rule and update members accordingly.
Legislative Update - March 10, 2023
 IHA Legislative Agenda
IHA Legislative Agenda
This week marked the beginning of the second half of the 2023 legislative session, which must adjourn by April 29. IHA’s agenda bills, HB 1460 and SB 400 have been assigned to committees in their second chamber, and IHA’s legislative team is actively working to ensure hearings for each bill. HB 1460, which modernizes the Indiana Professional Licensing Agency’s licensing process, has been assigned to the Senate Health & Provider Services Committee, and SB 400, which aligns state and federal medical error reporting requirements, provides prior authorization relief, streamlines the credentialing process, and enhances insurer premium transparency, has been assigned to the House Public Health Committee. IHA will keep you updated as these bills progress in the second half.
 Substance Use Disorder Treatment Plans
Substance Use Disorder Treatment Plans
On Wednesday, March 8, the Senate Health & Provider Services Committee heard HB 1462, which, as it passed the House, required each hospital emergency department to submit a substance use disorder treatment plan to the Indiana Department of Health for the subsequent year to initiate interventions with patients who have a substance use related emergency department visit. Rather than requiring a substance use disorder treatment plan, the Senate Health & Provider Services Committee amended the bill to require each emergency department to assess its ability to implement a substance use disorder treatment plan. As amended, the bill passed the Senate Health & Provider Services Committee by a vote of 10-0 and was recommitted to the Senate Appropriations Committee. IHA will continue to work on the legislation to ensure that substance use disorder treatment resources are available to patients while not overburdening our state’s emergency departments.
 Medicaid Rate Review
Medicaid Rate Review
On Thursday, March 9, the Indiana Family & Social Services Administrative (FSSA) presented the agency’s budget proposal to the Senate Appropriations Committee.FSSA's presentation includes the agency’s priority to build a statewide crisis response system. The agency also provided an overview of its intent to develop a rate review schedule to review Medicaid reimbursement rates for providers at least every four (4) years. The first tranche of rate review will include:
-
Home health
-
Dental
-
Non-emergency medical transportation
-
The various waiver programs that provide home and community-based services that coincide with FSSA’s managed long-term services and support initiatives
IHA will advocate for a rate review of hospitals to be included in one of the subsequent tranches and will continue to advocate for further Medicaid assistance in this year’s biennial budget.
Legislative Update - March 3, 2023
 Legislature Reaches Session Halftime
Legislature Reaches Session Halftime
This week marks the halfway point of the legislative session. All bills have made their way through their chamber of origin: Senate bills through the Senate, and House bills through the House. If a bill has not been voted on in its chamber of origin by this point, it is considered "dead" and will not advance further. However, there is an opportunity for language from dead bills to be revived and placed into bills that are still moving via an amendment. The IHA team will continue to be vigilant in fighting against any harmful language being added to bills.
A helpful tool for determining whether bills are still working through the process is the
Indiana General Assembly website. The website provides a complete list of bills filed this session. Bills listed in blue font are still alive and going through the process. Bills that have failed to advance and are effectively "dead" are in grey font.
 Status of Concerning Bills
Status of Concerning Bills
The legislature filed several bills this session that pose concerns to the health care community. Chief among those are two agenda bills in the Senate: Senate Bill (SB) 6 and SB 7, and two agenda bills in the House: House Bill (HB) 1003 and HB 1004.
The IHA team has worked diligently with legislators and stakeholders to agree on the language in each bill. At the halfway point of session, negotiations are ongoing, and progress is positive.
HB 1003: This bill initially contained harmful language that would have prohibited a health care provider from negotiating with a health carrier for reimbursement greater than 10% compared to any other health carrier for any service provided.
This harmful language was removed from the bill via amendment. Currently, the bill contains a health reimbursement arrangement tax credit, which would allow a credit against an employer's state tax liability for employers with less than fifty employees if the employer has adopted a health reimbursement arrangement in lieu of a traditional employer-provided health insurance plan. Additionally, the bill allows health care providers and health plans to enter into arrangements to reduce prior authorization burdens if a health care provider enters into a value-based contract and an electronic medical record access agreement with a health plan.
HB 1004: This bill initially contained harmful language that would have set rates for nonprofit hospitals at 260% of Medicare and created a penalty for exceeding that rate, as well as a ban on physician non-compete agreements with nonprofit hospitals and harmful site of service language.
After being amended in committee, HB 1004 no longer contains these harmful provisions. Instead, the bill includes a new Health Care Cost Oversight Board that will collect data about and oversee the cost of health care for hospitals, insurance companies, and the pharmaceutical industry. The bill also requires hospitals to reach national average prices or otherwise be assessed a penalty by the Indiana Department of Insurance starting in 2026. IHA believes that the language in HB 1004 represents Indiana hospitals' commitment to health care affordability and the partnership between hospitals and the Indiana legislature. The IHA team will continue working toward additional solutions in collaboration with the legislature and other stakeholders as this bill progresses.
SB 6: This bill contains site of service language that would be devastating to hospitals by prohibiting hospitals from recovering facility costs for any outpatient services. Although the Senate Committee on Health and Provider Services heard extensive testimony on the harm this bill would cause hospitals, the Senate advanced the bill by a vote of 30-18. The IHA team continues to advocate against this legislation and will work hard to ensure the language in this bill does not pass the House during the second half of session.
SB 7:
This bill passed through the Senate a few weeks ago and contained a complete ban on physician non-compete agreements with employers. Similar to SB 6, the Senate refused to change the prohibition in the bill, instead sending it to the House for further consideration of the policy. IHA has continued to work toward an acceptable compromise in the discussion of physician non-compete agreements and is working toward a solution that will be acceptable to hospitals as the session progresses.
Bills that did not advance through the first half of session that would have impacted hospitals include:
-
A wrongful death proposal.
-
Legislation that would add to the reporting requirements for hospitals.
-
A bill to expand upon the public forum requirements.
Thank you for your advocacy with your local legislators on behalf of your hospitals. Although some of the bills harmful to hospitals are continuing through the process, your advocacy is making a difference. Legislators are hearing and understanding the concerns, and we believe there is still an opportunity to stop harmful legislation. So again, thank you for your continued support, and please continue to communicate with your legislators your concern with these bills as the second half of session begins.
 IHA Legislative Agenda Update
IHA Legislative Agenda Update
While defending against legislation that would harm Indiana hospitals and negotiating a beneficial path forward, the IHA team has also been lobbying for a proactive agenda of legislation to improve health care access in Indiana and support health care providers across the continuum of care.
HB 1460:
This legislation would create additional flexibility for licensing boards to convene for business and helps modernize the Professional Licensing Agency's (PLA) licensing process. The goal is for PLA to issue all licenses within 30 days and ensure Indiana's licensing process is not a barrier for individuals entering the health care workforce. To that end, the bill requires PLA to issue full reciprocal licenses within 30 days so long as one license from another state can be verified in that timeframe.
The bill also requires PLA to issue notifications to individuals if their applications are incomplete to assist in expediting the application process.
This legislation passed through the House and has been sent to the Senate for further consideration.
SB 400:
This legislation would require an insurer to submit written justifications to the Indiana Department of Insurance (IDOI) for premium increases, which would then be available publicly. This change ensures transparency in insurer premiums, providing additional insight into Indiana's health care cost drivers.
The bill would also:
-
Require urgent PA determinations to be made within 48 hours and nonurgent PA determinations to be made within five business days;
-
Require a health plan to provisionally credential a provider within 15 days;
-
Require peer-to-peer reviews for adverse determinations;
-
Prohibit a clean claim from being altered to only pay for the CPT codes necessary for an individual's final diagnosis if the CPT codes were medically necessary to reach the final diagnosis;
-
Require full reimbursement rate schedules to be provided;
-
Align the state's medical error reporting requirements with the National Quality Forum, so there is not a difference in reportable events; and
-
Extend the time period for medical staff appointments and reappointments to three years to align with the Joint Commission.
Additionally, the bill creates a pilot program with the State Employee Health Plan that would prohibit insurers from requiring prior authorization for a certain number of often-approved CPT codes.
This bill passed through the Senate and will now be considered in the House.
HB 1059: This bill would enhance criminal penalties for those convicted of assault against individuals who work in emergency departments. The enhanced criminal penalties would match those applied to individuals who assault police officers and the criminal penalties already in Indiana Code for certain health care professionals.
This bill did not get a hearing in the House during the first half of session. This was due to concern about expanding the criminal code to cover all the additional people employed by emergency departments across the state. Although the bill has yet to progress, the IHA team will continue to advocate on behalf of this concept during the second half of session to pass this concept by the end of the legislative session.
Legislative Update - February 24, 2023
 HB 1004 Amended in Committee
HB 1004 Amended in Committee
The House Committee on Public Health considered House Bill (HB) 1004 for a second time on Monday. The committee did not hear public testimony, having already heard extensive testimony during the first hearing. The committee adopted an amendment to HB 1004 that removed the language requiring hospitals to charge 260% of Medicare or less, as well as the language banning noncompete agreements between physicians and not-for-profit hospitals, the harmful site of service provisions, and the provisions prohibiting certain employment arrangements and contractual provisions with insurers. The amendment included the creation of a Health Care Cost Oversite Board, which would consider the prices hospitals charge for services compared to the national average, and gives the Indiana Department of Insurance authority to enforce a penalty beginning in 2026 if hospitals are found to exceed the national average price for services. The amendment also includes a tax credit for new physicians starting independent practices in the state. The full text of the amended legislation can be found here.
HB 1004 was passed by the committee and sent to the full House for consideration. One second reading amendment was discussed in the House but ultimately not adopted, and the House will have a third reading vote (final vote in the House) next week. If the bill passes on third reading, it will be sent to the Senate for consideration.
IHA Agenda Legislation Advances
HB 1460, which would streamline the professional licensure process for health care professionals, passed unanimously out of the House this week and will now be sent to the Senate for further consideration. This bill will contribute to alleviating the health care workforce challenges Indiana currently faces.
Senate Bill (SB) 400 passed the Senate Appropriations Committee this week. It will be considered for second and third reading in the Senate next week before being sent to the House for further consideration. SB 400 contains a pilot program for the state employee health plan to require automatic prior authorization approvals for the most often approved CPT codes. It also requires insurers to explain the reasoning behind yearly premium increases to policyholders. The bill also streamlines credentialing across Medicaid and commercial health plans and requires commercial health plans to provide health care providers with full reimbursement rate schedules.
 House Approves Budget, Sends to Senate
House Approves Budget, Sends to Senate
The House considered their version of the state’s biennial budget, HB 1001, this week in committee, then voted to pass it and send it to the Senate for further consideration. The budget includes an 11% increase in K-12 education funding over the biennium for $1.6 billion and tax cuts that would save Hoosiers an estimated $625 million over the biennium.
The budget includes $225 million for the Governor’s requested public health funding. The amount is less than the Governor initially requested but significantly increased from the $7 million per year previously allocated for county health departments. The budget also contains $10 million for regional mental health facility grants, increasing Medicaid reimbursement for physicians from 83% of Medicare to 90%. The current budget version also reduces the percentage of HAF fees that the state takes for HIP administration from 28.5% to 26%, and instead reallocates that money back to hospitals. That is a modest decrease, but the House has confirmed it is a placeholder for further discussions. IHA will continue to advocate for Medicaid and HAF relief as the budget makes its way through the Senate.
 Legislature Nears First Half Deadlines
Legislature Nears First Half Deadlines
The legislative session calendar is effectively broken into two halves. During the first half of session, bills make their way through their chamber of origin: Senate bills through the Senate, and House bills through the House. To ensure bills move through the process on time, the legislature has deadlines for considering bills. This week was the deadline for bills to be considered in committees. Next week is the deadline for bills to be considered on second and third readings.
If bills are considered in their respective chambers before these deadlines, they are sent to the other chamber for further consideration. Bills that do not advance through the process in the first half of session are considered “dead,” but the language may be added to a bill that did pass either chamber via an amendment.
Legislative Update - February 17, 2023
 House Committee Considers Multiple Health Care Bills
House Committee Considers Multiple Health Care Bills
The House Committee on Public Health considered multiple health care-related bills this week. House Bill (HB) 1433 requires Medicaid reimbursement for orthotic devices. The bill also addresses concerns with Medicaid reimbursement related to prosthetic and orthotic devices for children. It specifies that a minor may receive a prosthetic or orthotic device for their medical needs and a device for recreational activities. Many individuals testified in support of the bill, explaining the need for an improved reimbursement structure for these devices, especially when they are being provided to children who grow quickly and need new devices often. The bill passed the committee unanimously.
The committee also unanimously passed HB 1568, which deals with prescriptions for hormonal contraceptives. The bill would allow pharmacists who meet specific requirements to prescribe and dispense hormonal contraceptive patches and self-administered hormonal contraceptives. A pharmacist is not required to prescribe a contraceptive if the pharmacist believes it is contraindicated or if the pharmacist has ethical, moral, or religious objections to prescribing. This bill is one of the multiple proposals being considered in both the House and Senate this year dealing with access to contraception.
 Senate Health Committee Passes IHA Priority Bill, Discusses Others
Senate Health Committee Passes IHA Priority Bill, Discusses Others
The Senate Committee on Health and Provider Services unanimously passed Senate Bill (SB) 400 on Wednesday. This bill, authored by Senator Liz Brown (R-Fort Wayne), would require insurers to provide an explanation of premium rate increases to their plan holders, as well as create a pilot program to prohibit the CPT codes most often approved via prior authorization from being subject to prior authorization requirements for a 3-year period. This pilot would be an essential step toward alleviating the challenges prior authorization poses to the provider community. The bill now goes to Senate Appropriations for further consideration.
The committee also discussed but did not vote on SB 378, legislation that would adjust the Hospital Assessment Fee (HAF) program in Indiana. Alan Fisher, CEO of Woodlawn Hospital, attended the committee to explain to members the impact of increasing HAF fees on his hospital and the benefits HAF has provided in increased reimbursement. Congresswoman Victoria Spartz (pictured speaking to Brian Tabor) also attended the hearing to comment on the HAF program. The committee heard testimony from various viewpoints but ultimately did not vote on the legislation. IHA will provide further updates on the status of the bill as they become available. IHA is continually grateful for our member's participation in the legislative process by engaging with legislators through meetings, testimony, and other communication of hospital priorities.
 House Considers Amendments to Health Agenda Bills
House Considers Amendments to Health Agenda Bills
On Tuesday, the House Committee on Insurance made changes to HB 1003. Most notably, the concerning contract language that required a health care provider to ensure all contracts with all health carriers were within 10% of each other for each service provided was removed from the bill. Rob McLin, CEO of Good Samaritan Hospital (pictured) previously testified before the committee that the bill's contracting provision would harm negotiations between hospitals and payers. The removal of the language ensures that hospitals and payers are free to contract without interference. The amendment also added language that says a health care provider entering into a value-based health care reimbursement arrangement and an electronic medical record access agreement with a health plan may qualify for participation in a program to reduce or eliminate prior authorization requirements. The committee passed the bill with the changes, and the House Committee on Ways and Means will now consider it.
HB 1004, which currently contains language that would cap reimbursement rates for not-for-profit hospitals at 260% of Medicare, is set to be considered for a second time on Monday morning in an extra meeting of the House Committee on Public Health. IHA is continuing to advocate for the harmful provisions in HB 1004 to be removed and will keep you updated on the progress of the legislation.
Legislative Update - February 10, 2023
 Senate Committee Considers Site of Service Bill
Senate Committee Considers Site of Service Bill
The
Senate Committee on Health and Provider Services discussed and voted on
Senate Bill (SB) 6this week, which contains site of service requirements. Specifically, the legislation would require a provider to submit bills for health care services in an office setting on an individual provider form only, and would prohibit the use of an institutional provider form. As written, the term “office setting" includes health care services that are provided on an ambulatory basis even if they are provided within the four walls of a hospital.
IHA President Brian Tabor testified in opposition to this legislation, explaining IHA members' concerns with the language. He noted that contracts between hospitals and insurers are already negotiated to include approved sites of care and associated pricing, and SB 6 would override these contracts. Tabor also pointed to the low reimbursement of physicians in Indiana that has led to hospital employment of physicians in order to improve physician reimbursement opportunities. Gregg Ferlin, CFO at Community Healthcare System, and Jeffrey Costello, Chief Financial Officer at Beacon Health System, also testified on behalf of IHA in opposition to the legislation. They both explained that the legislation would impact their hospitals in the amount of tens to hundreds of millions of dollars per year and result in closures of service lines and entire hospitals.
The committee voted to pass the bill out of committee by a vote of 8-4. Senator Charbonneau, who chairs the committee and is also the author of the bill, recognized the extensive concern that both stakeholders and committee members had with the bill and promised to hold the bill on second reading until legitimate concerns with the bill are alleviated and the harmful risk to access to care is significantly limited.
Please continue to share your concerns about SB 6 with your local legislators.
IHA will continue to advocate against the passage of SB 6 and other harmful legislation, while continuing to negotiate a meaningful path forward to national average prices and asking the legislature to address other areas of the health care industry that also drive cost, including insurance and pharmaceuticals.
If you would like to view the committee discussion, you can do so
here.
The committee took place at 9:00 a.m. on February 8 and the discussion of SB 6 begins at 1:17:00.
Licensing Modernization Bill Passes House Committe e
e
House Bill (HB) 1460, which modernizes the licensure processes at the Indiana Professional Licensing Agency (PLA), was passed unanimously by the
House Committee on Employment, Labor and Pensionson Thursday. The bill would allow PLA licensing boards to meet virtually to ensure meetings to review and approve licenses are not canceled due to quorum issues and sets a timeframe within which board vacancies must be filled. The bill also streamlines the reciprocity process as well as requires PLA to report on timelines for license issuance with the goal of timely licensure for all professions in the state.
Sergio Cianci Chapman, CEO of Valle Vista Health System, testified in support of the legislation. He explained to the committee that his organization has a difficult time filling vacancies for behavioral health professionals due to Indiana's slow licensing process and said this bill would alleviate the workforce shortage he is facing.
A product of an IHA-sponsored workforce summit in 2022, this legislation is a collection of recommendations to improve and expand Indiana's healthcare workforce pipeline. The bill will now continue through the process and be considered by the full House.
 Noncompete Ban Still Being Considered
Noncompete Ban Still Being Considered
After being voted out of the Senate health committee last week,
SB 7, which would ban noncompete between physicians and their employers, was considered by the full Senate. IHA worked diligently with the bill author and other stakeholders to come to a mutual agreement on the bill. However, the author decided not to consider any changes at this time, and instead, the bill was passed through the full Senate by a vote of 45-5. Although this was a disappointment, IHA remains committed to working toward a compromise that will be acceptable to all sides of the discussion, in addition to working toward a broader agreement of bringing hospital prices in line with the national average in the larger conversation about healthcare costs. The IHA team is grateful for the feedback of our members on this issue and urges that you continue to provide feedback to your local legislators about your concerns with this legislation as it moves to the House for further consideration.
Legislative Update - February 3, 2023
 Hospital CEOs Testify on House Bill 1004
Hospital CEOs Testify on House Bill 1004
The House Committee on Public Health heard testimony on House Bill (HB) 1004, which contains provisions that would harm hospitals if passed. Among the provisions is one that would prohibit a hospital from charging a price of more than 260% of Medicare for any service provided; otherwise, the state will levy a fine on the hospital. The bill also contains site-of-service contract interference provisions and a ban on physician non-compete agreements. Multiple organizations testified in support of the requirements, including the Employers Forum and Hoosiers for Affordable Healthcare.
Brian Tabor, President of the Indiana Hospital Association, testified in opposition to the legislation. In his testimony, he shared that Indiana hospital systems are committed to partnering with state leaders in reaching the national average in prices. Still, the provisions in HB 1004 would make that achievement impossible.
Bryan Mills, CEO of Community Health Network, testified in opposition to the bill, making it clear that the 260% cap on negotiated prices would negatively impact hospitals for many reasons, including because Medicaid reimbursement is only 53% of the cost of providing care, resulting in the need to shift costs to keep hospitals open. He suggested that an increase in Indiana's Medicaid base rate would be a helpful way to lower commercial costs by improving government reimbursement.
Mike Schroyer, CEO of Baptist Health Floyd in New Albany, Indiana, also testified in opposition to the bill. He cautioned the committee against passing the bill because it would have unintended consequences. In addition, he urged against passing the site of service provisions and instead allowing independent entities the freedom to contract.
Terry Metzger, System COO of Ascension Indiana, testified in opposition to the bill, and shared alternative ways to lower health care costs in Indiana. In addition, he discussed the work Ascension St. Vincent is doing to create direct-to-employer contracting opportunities, removing the middleman and giving employers insight into and impact on the employee health contracts.
The committee did not vote on the bill this week, instead holding it for further consideration and discussing possible amendments. IHA will update the bill's status as information becomes available.
If you would like to view the recording of the committee, you can view it at this link.
The committee took place on January 31, 2023. The discussion of HB 1004 began at 42:51, and IHA testimony began at 3:01:15.
House Insurance Committee Considers Bill Impacting Hospitals
The House Committee on Insurance considered HB 1003 this week. This bill contains a provision that says a health provider facility may not enter into a contract with a health carrier that would result in reimbursement to the health provider facility for any service that is greater than 10% of the reimbursement the provider receives for that service from any other health carrier.
Rob McLin, CEO of Good Samaritan Hospital in Vincennes, Indiana, testified in opposition to the bill. He acknowledged that the bill's goal to improve competition among insurance carriers was good. Still, McLin said the execution of that goal in the bill was actually harmful to hospitals rather than accountability for insurance companies. He said that when a rate cap is placed on reimbursement, as this bill would do, the rate floor is effectively raised for all carriers. The effect would be that all of a hospital's health carrier contracts would have to fall within 10% of each other—and in order for a hospital to get the rate needed from one, all the others have to come up and match that rate.
Instead of government-set rate caps, he encouraged the committee to consider creating incentives for direct-to-employer contracting and strengthening the bill's provision that would give a tax credit to employers who utilize alternative employee health reimbursement arrangements.
The Insurance Committee also heard Hoosiers for Affordable Healthcare testimony supporting the legislation. As a result, HB 1003 was held for further consideration and possible amendments and is expected to be further discussed in a future committee meeting.
If you would like to hear Rob McLin's testimony, you can find the committee hearing on HB 1003 at this link.
The video is under February 1, 2023, and the discussion of HB 1003 begins at 41:30.
 Public Health Funding Bill Heard in Senate Health Committee
Public Health Funding Bill Heard in Senate Health Committee
Senate Bill (SB) 4,
which would provide funding to local health departments, was passed out of the Senate Committee on Health and Provider Services this week. The legislation will now be considered by the Senate Committee on Appropriations, given its fiscal impact, before advancing to the full Senate for consideration.
The legislation results from the recommendations given by the Governor's Public Health Commission, which was created to assess and improve Indiana's public health infrastructure. IHA President Brian Tabor and other leaders in Indiana's health care community participated in the commission to make the recommendations.
Legislative Update - January 27, 2023
 Senate Health Committee Discusses Non-compete Agreements
Senate Health Committee Discusses Non-compete Agreements
The Senate Committee on Health and Provider Services met this week to consider multiple bills, including Senate Bill (SB) 7,
which would ban non-compete agreements between hospitals and physicians.
The committee heard testimony in favor of and against banning non-compete agreements for physicians. If the bill passes, it would prohibit a physician and an employer from entering into a non-compete agreement beginning July 1, 2023. Dr. Eric Fish, President, and CEO of Schneck Medical Center, testified against the bill on behalf of IHA. Dr. Fish expressed the important purpose non-compete agreements serve for employers to protect the time and capital invested in employees, and to preserve access to and continuity of care in a community. Dana Stutzman, a health law attorney with Hall Render, also testified on behalf of IHA, sharing the legal reasoning between physician non-compete agreements, and cautioning that banning these non-compete could result in higher healthcare costs. The Indiana Chamber and the Indiana Rural Health Association also testified against the bill.
Despite strong opposition to the bill expressed in public testimony, the committee voted to pass the bill by a vote of 9-3. The author, Senator Justin Busch, committed to considering amendments to the bill that would help rural hospitals. Details of such amendments are not yet known, but more information is expected next week. In addition, IHA will continue to work to preserve the ability for hospitals and physicians to freely contract with each other, including preserving non-compete agreements.
 Bill to Streamline Credentialing, Prior Authorization, Heard in Senate Health
Bill to Streamline Credentialing, Prior Authorization, Heard in Senate Health
SB 400, authored by Senator Liz Brown (R-Fort Wayne), was also discussed in the Senate Committee on Health and Provider Services this week. The bill contains several provisions to streamline health care delivery. Among these are provisions to improve the credentialing process between physicians and managed care organizations (MCOs). For example, the bill would require an MCO to issue a credentialing determination no later than thirty calendar days after the provider submits a complete credentialing application, or otherwise issue a temporary credential.
The bill also contains provisions to improve the prior authorization process. These provisions include specifications on peer-to-peer review requests, requirements for health plans to notify providers of technical issues with the prior authorization submission process, and prohibiting health plans from requiring prior authorization of drugs that previously did not require the process for the duration of the policy contract. IHA is also advocating for additional prior authorization improvements to be included in the bill through an amendment, including a pilot program that would prohibit prior authorization of specific CPT codes that are often approved.
In addition to the prior authorization and credentialing streamlining, the bill contains language requiring insurers to explain their premium increases to the Indiana Department of Insurance each year. These changes would be an effective step toward total transparency of health care costs, in line with what hospitals already provide through price transparency. The bill also requires insurers to provide their full reimbursement rate schedule and update it when three or more CPT codes change in a year.
Julie Slinker, Senior Director of Revenue Cycle from Rush Memorial Hospital, testified in support of the bill on behalf of IHA. The committee did not vote on the bill this week due to the extensive contents and plans to include additional changes. The bill is expected to be considered in committee again next week before being voted on.
IHA is grateful for the testimony of all of our members in health committee this week!
 Public Health Day Gathers Crowd
Public Health Day Gathers Crowd
Hundreds gathered at the Indiana Statehouse on Thursday to support Public Health Day. The event's goal was to publicize the work being done across Indiana to improve the state's public health services, and to advocate for public health legislation making its way through the legislative process.
The event featured Governor Eric Holcomb, State Health Commissioner Dr. Kristina Box, and other prominent public health advocates in the state to discuss the importance of public health funding and initiatives. The Statehouse was filled with advocates wearing blue and gold, eager to hear and spread the message of health improvement. IHA was grateful to participate in the event, with many IHA staff from various departments in attendance. A special thanks to member hospitals who came to support the day. We appreciate your advocacy on this critical issue.
Legislative Update - January 20, 2023
 Hospitals Still Need Your Help
Hospitals Still Need Your Help
Thank you for your advocacy on behalf of your hospital over the last week. Legislators have heard from their constituents around the state about the harm to hospitals if legislation that interferes with private contracts and creates government rate setting in health care markets is allowed to pass.
The IHA team has been meeting with legislative leadership to explain the detrimental effects of the legislation and will continue to advocate on behalf of Indiana hospitals. However, we still need your help. As the legislature continues to consider the harmful provisions in Senate Bill (SB) 6, SB 7, HB 1003, and HB 1004, please make your voice heard.
Reach out to your representatives and senators, tell them about your concerns with this legislation, and ask them to vote "no."
Click the button below to send a pre-written message directly to the legislators who represent your district. Estimated time, 2-3 minutes.

Here's how it works:
-
Click the red button below to open the IHA Action Center.
-
Once open, there will be a sample message drafted in the Message Body section —feel free to customize this message to reflect your individual hospital.
-
Next, fill out your contact info in the boxes below the Message Body section.
-
Once complete, hit the blue “send message” button to ensure your voice is heard. You will receive a confirmation email notifying you that your message was successfully sent and to which legislators. Note: First-time users will need to authenticate by verifying their email. Be sure to check your junk/spam if you do not see that message.
 Not-for-profit Public Forum Bill Heard in Committee
Not-for-profit Public Forum Bill Heard in Committee
The House Committee on Public Health met for the first time in 2023 this week to hear presentations on public health from state agencies and consider bills. In addition, the committee heard testimony on House Bill (HB) 1271, which addresses nonprofit hospital and insurer reporting. Specifically, this bill would increase the requirements on the public forums that not-for-profit hospitals and insurers are required to hold yearly.
The additional requirements include posting notice of the meeting at least forty-five days in advance of the forum, and allowing remote attendance of the forum through real-time audio and video over the internet. Additionally, the forum presentation must contain financial statements for the preceding three years, including organization income statements, balance sheets, and cash flow statements, and a discussion of the pricing of inpatient and outpatient health services provided by nonprofit hospitals and their affiliates.
Due to time constraints, the committee did not vote on the bill this week. Instead, the bill will be considered again next week to allow for additional testimony. IHA President Brian Tabor will testify on the bill next week to express IHA's concerns with the bill.
 IHA Agenda Bills Filed
IHA Agenda Bills Filed
The bills that contain IHA's proactive legislative agenda have all officially been filed and can now make their way through the legislative process. Although the many threats to hospitals take up much of our communication with members, these bills deserve recognition, given their urgency. IHA will continue to advocate for their passage and implementation throughout session.
Licensing Modernization
HB 1460 addresses professional and occupational licensing. Authored by Rep. Brad Barrett, this legislation will streamline the licensure process for health care professionals, ensuring they can begin caring for patients as soon as possible.
Workforce Pipeline
HB 1216 provides funding for the development of health professions. Specifically, the bill creates the Linking Industry to Nursing Education (LINK) fund and offers additional resources to the Professional Licensing Agency for improved license issuance. This legislation is authored by Rep. Ethan Manning.
Health Insurance Transparency and Prior Authorization Streamlining
SB 400 deals with health care matters. Specifically, this legislation would improve health care cost transparency by requiring an insurer to submit a written justification to the Indiana Department of Insurance (IDOI) if their proposed premium increase is 5% or more than the previous year's. Additionally, the bill creates a pilot program banning insurers from requiring prior authorization for a certain number of often-approved CPT codes. Sen. Liz Brown authored this legislation.
Protections for Health Care Workers
HB 1059 provides protections for emergency medical service providers. This bill would enhance criminal penalties for those convicted of assault against individuals who work in emergency departments. The enhanced criminal penalties would match those applied to individuals who assault police officers and the criminal penalties already in Indiana Code for certain health care professionals.
 IDH: Public Health Day
IDH: Public Health Day
The Indiana Department of Health is holding Public Health Day at the Statehouse on January 26th. All are welcome to come to the Statehouse and show their support for Indiana public health. For more information,
 download the flyer or click here.
download the flyer or click here.
Legislative Update - January 13, 2023
 House Republican Legislative Agenda Targets Hospitals
House Republican Legislative Agenda Targets Hospitals
House Speaker Todd Huston (R-Fishers) announced the
House Republican legislative agenda for the 2023 session yesterday. The agenda includes the following:
-
Investments in education initiatives, including school choice.
-
Funding for economic development and mental health treatment.
-
Affordable housing and childcare investments.
-
An effort to lower health care costs and increase market competition.
We Need Your Help
While lowering health care costs is a goal the Indiana Hospital Association (IHA) shares, the methods the House Republicans have proposed are harmful and heavy-handed government interference in the health care market. Therefore, the Indiana Hospital Association (IHA) is taking swift and continued action to oppose these adverse pieces of legislation.
We ask for your assistance in expressing your concern to legislators. Please tell your legislators you are not happy with their efforts to harm Indiana hospitals and interfere in private contracts. Tell them to vote "no" on
HB 1003 and
HB 1004 in the House and
SB 6 and
SB 7 in the Senate. Read more details below.
Click the button below to send a pre-written message directly to the legislators who represent your district. Estimated time 2-3 minutes.
Here's how it works:
-
Click the red button below to open the IHA Action Center.
-
Once open, there will be a sample message drafted in the Message Body section —feel free to customize this message to reflect your individual hospital.
-
Next, fill out your contact info in the boxes below the Message Body section.
-
Once complete, hit the blue “send message” button to ensure your voice is heard. You will receive a confirmation email notifying you that your message was successfully sent and to which legislators. Note: First-time users will need to authenticate by verifying their email. Be sure to check your junk/spam if you do not see that message.
IHA President Brian Tabor expressed dismay at these legislative goals in an
Indianapolis Business Journal article published yesterday. "This level of government control is an extreme departure from Indiana's free market principles. Hoosiers do not want more government interference in health care, and we have not seen the government picking winners and losers to this extent since Obamacare. If legislative leaders are looking for real solutions, they should start by raising state Medicaid rates– which only cover 53% of hospitals' cost of providing care – to relieve the cost-shifting burden on businesses and consumers."
Government Contract Interference
House Bill (HB) 1003, titled health matters, offers two seemingly helpful solutions. These are prior authorization reform, popularly known as "gold card" language, and an employer tax credit for employers using alternative methods of employee health insurance. Though these two provisions seem helpful, the central portion of this bill sets a government-imposed cap on the payments hospitals are allowed to receive from insurance companies for care provided. In addition, in negotiations between health care providers and insurers, hospitals are not allowed to negotiate with any payor above 10% of the price included in their lowest-reimbursed contract. This government interference in private contracts and contract negotiation cannot be tolerated. IHA opposes HB 1003 because of this language, which will hurt every hospital in the state with no hope of saving any money for consumers.
Government Rate Setting
HB 1004, titled health care matters, contains a raft of harmful provisions hindering health care delivery in the state. The provisions of most significant concern are as follows: First, the bill includes a fine for nonprofit hospitals (excluding county-owned and CAHs) that charge more than 260% of the Federal Medicare reimbursement rate for health care services. This provision amounts to government rate setting, denying health care providers the ability to negotiate the rates they are paid for their services. The bill also imposes "site of service" restrictions on hospital billing structures, denying hospitals the ability to charge the necessary rate for services to allow them to cover costs. This language mirrors language found in
Senate Bill (SB) 6, which is also of great concern to IHA.
Further, HB 1004 restricts a health care provider's ability to contract with an insurer, imposing limitations on what types of provisions may be included in a contract negotiated between private entities. HB 1004 also prohibits nonprofit hospitals (excluding CAHs and county-owned hospitals) from entering into or changing physician noncompete agreements after July 1, 2023. This language also mirrors Senate language found in
SB 7. For these reasons, IHA opposes HB 1004.
Again,
please click here to send a message directly to the legislators who represent your district.
 IHA Proactive Legislative Agenda
IHA Proactive Legislative Agenda
The first week of the 2023 Indiana Legislative Session was packed as the
IHA Government Relations team has already established efforts to fend off attacks on hospitals from both the House and the Senate.
While defending against legislation that would harm Indiana hospitals, the IHA team is also lobbying for a proactive agenda of legislation that would improve health care access in Indiana and support health care providers across the continuum of care.
Licensing Modernization
Author: Rep. Brad Barret (R-Richmond)
This legislation would create additional flexibility for licensing boards to convene for business and establishes the Professional Licensing Agency (PLA) to modernize the agency's licensing process. The goal is for PLA to issue all licenses within 30 days and ensure Indiana's licensing process is not a barrier for individuals entering the health care workforce.
Workforce Pipeline
Author: Rep. Ethan Manning (R-Logansport)
This bill will create the Linking Industry to Nursing Education (LINK) Fund, administered by the Commission for Higher Education, which will be used to match investments by health care entities in nursing education programs. The bill also requires the state to allocate additional resources to PLA to operate, understanding that increased funding to pay for technology and employees will result in improved licensing turnaround times.
Health Insurance Transparency & Prior Authorization Streamlining
Author: Sen. Liz Brown (R-Fort Wayne)
This legislation would require an insurer to submit a written justification to the Indiana Department of Insurance (IDOI) if their proposed premium increase is 5% or more than the previous year's increase. The change ensures transparency in insurer premiums, providing additional insight into Indiana's health care cost drivers. The bill will also prohibit denials of requests for prior authorization if the request is for a medically necessary service. Additionally, the bill creates a pilot program banning insurers from requiring prior authorization for a certain number of often-approved CPT codes.
Protections for Health Care Workers
Author: Rep. Karen Engleman (R-Georgetown)
This bill would enhance criminal penalties for those convicted of assault against individuals who work in emergency departments. The enhanced criminal penalties would match those applied to individuals who assault police officers, as well as the criminal penalties already in Indiana Code for certain health care professionals.
The IHA team will continue to provide updates on bills of interest or concern as the legislative session progresses.
Please click here to see a list of bills of interest and their current legislative status.
 Governor Holcomb Gives State of the State Address
Governor Holcomb Gives State of the State Address
On Tuesday,
Governor Holcomb gave his annual State of the State Address to the legislature and other leaders from across Indiana. The Governor's speech focused on the state's achievements across the board and highlighted three areas for focusing on future growth.
These three areas were securing Indiana's economic future, transforming public health delivery, and investing in pre-k through adult learning and education. Governor Holcomb requested funding for the Regional Economic Acceleration and Development Initiative (READI) as part of his economic goals. For education, the Governor asked for the state's most significant investment in education in the state's history, asking for a K-12 tuition support increase of more than $1.1 billion and a $184 million increase in higher education funding.
The Governor's focus on public health is the next step following the conclusion of his Public Health Commission, which released its recommendations last fall. Governor Holcomb requested the implementation of the commission's recommendations, including an increase in Indiana's public health appropriation to fund local initiatives and improve the delivery of public health services across the state's various rural, urban, and suburban areas.
To watch or read the Governor's full address,
please click here.
Legislative Update - January 6, 2023
 Governor Releases 2023 Agenda
Governor Releases 2023 Agenda
This week, Governor Holcomb announced his 2023 Next Level Agenda, which includes priorities for the legislative session and other areas of state government. The Governor focused on multiple policy areas, including health care policy. His health agenda items are as follows:
-Increase the annual appropriations to state public health in the state budget.
Specifically, the Governor is requesting $120 million in fiscal year (FY) 2023 and $227 million in FY 2024. Most of these dollars will be available to county officials to be used for the implementation of the various recommendations from the Governor’s Public Health Commission. These recommendations include core public health services in all 92 counties, a state health office of data and analytics for public health data, and improved access to child and adolescent health screenings, among other recommendations.
-Improve access to mental health services.
This improved access includes expanding 988 Crisis and Suicide Lifeline services, developing crisis stabilization units beginning with a pilot program, and working toward the Governor’s Challenge to Prevent Suicide among veterans and service members. These priorities and others will be addressed during the legislative session and through administrative action during 2023.
-Provide resources to combat the drug epidemic.
Governor Holcomb plans to launch a Treatment Finder Program to help Hoosiers connect with the appropriate addiction treatment. In addition, the state will receive more than $500 million from the national opioid settlement, which will be used to create more substance use programs to help Hoosiers struggling with addiction.
The Governor’s agenda also includes policy priorities in education and workforce, economic development, community development, and good government.
More information on the Governor’s agenda can be found here.
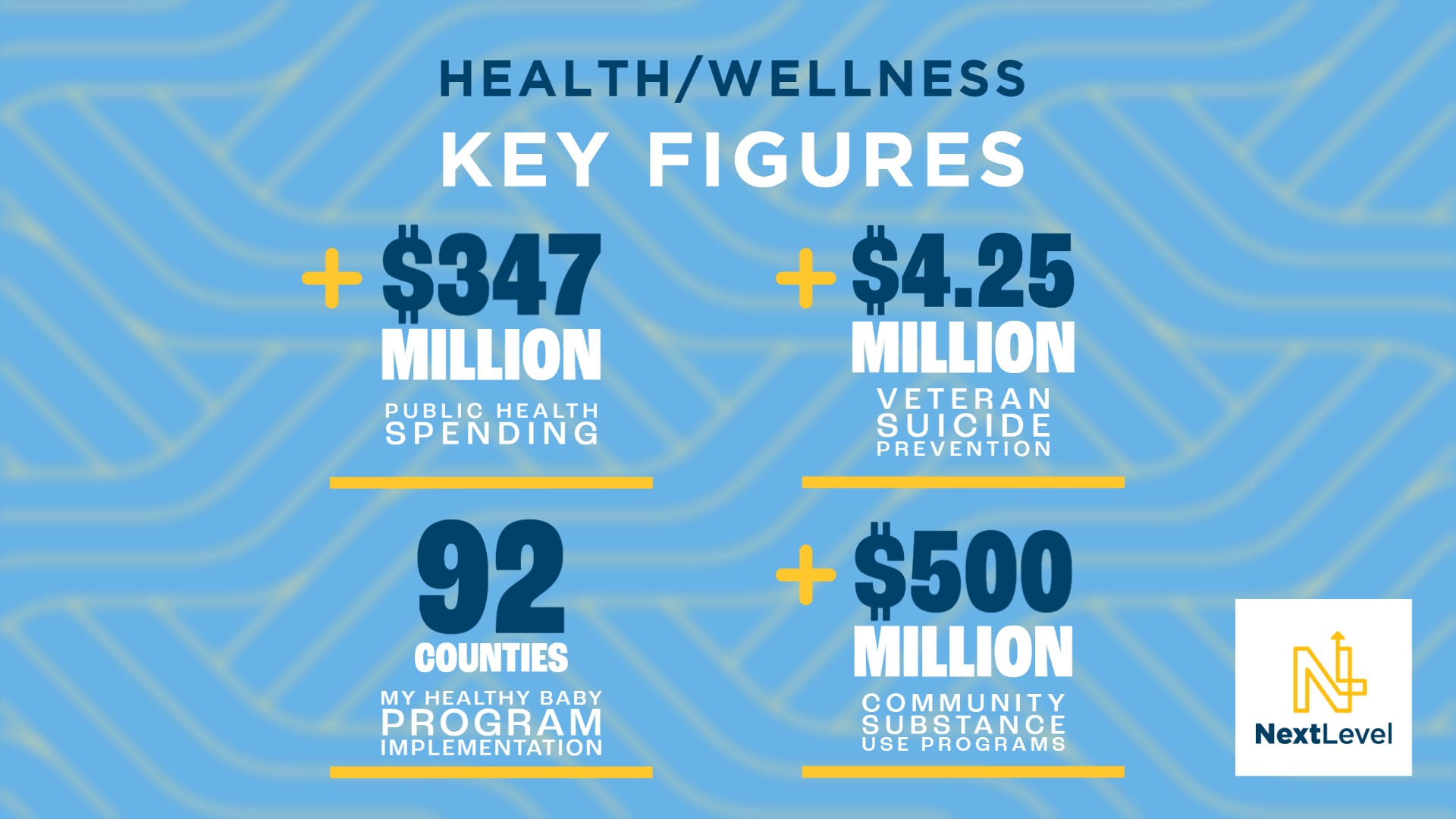
In addition to his agenda, Governor Holcomb also released his budget proposal for the 2023 legislative session. This budget is the Governor’s recommendation to the legislature for incorporating his policy priorities into the 2023 biennial budget, which the legislature will create beginning next week. The House and Senate are expected to release their legislative priorities and budget plans in the coming days as the 2023 legislative session gets underway.
The Governor’s proposed budget can be found here.
 Health Care Costs Expected Priority in 2023 Session
Health Care Costs Expected Priority in 2023 Session
A recent story in the Indiana Capital Chronicle provided insight into the expected prioritization of health care issues during the 2023 legislative session. The Governor’s Public Health Commission has brought public health funding back to the forefront of conversations after less discussion in previous years. In addition to this funding, lawmakers continue to express concern about the high cost of health care across the state and are looking for ways to use their legislative platforms to help lower those costs.
In light of this, IHA expects multiple pieces of legislation this session that address health care cost issues, some of which are likely to target hospitals. As session begins next week, it will be vital that legislators hear from their local hospitals about the health care concerns and cost drivers in their local communities.
How You Can Help: Please contact your area legislators and request meetings as soon as possible (either virtual or in person) to share with them what your hospital is doing to serve the community and how current economic circumstances impact your finances. If you’ve recently met with your legislators, thank you so much for doing so. Please continue to reach out to them and provide thoughts and helpful information. One way to begin the conversation is to reach out and mention that you saw the above Capital Chronicle article and want to talk about your concerns in that light.
Your legislators need to hear from you. As they gather at the statehouse, they are considering a vast array of issues in a short amount of time. The expertise and local connection you provide is vital as legislators make decisions. IHA’s government relations team is committed to advocating for hospital interests to the best of our ability. Still, there is no replacement for local hospitals reaching out to their representatives and senators.
The
IHA advocacy team will help you connect with your legislators and provide any talking points you need. Please do not hesitate to reach out for assistance.
Legislative Update - December 21, 2022
 Omnibus Spending Bill Released with Health Provisions
Omnibus Spending Bill Released with Health Provisions
Federal legislative leaders have unveiled details of the fiscal year 2023 Omnibus Appropriations legislation that will fund the government through September 30, 2023. The President is expected to sign the bill into law ahead of the Friday deadline when current government funding is set to expire.
The American Hospital Association (AHA) has released a breakdown of the legislation’s provisions related to hospitals and health systems. The legislation includes many provisions beneficial to hospitals, including preventing significant cuts to Medicare, extending essential programs set to expire this year, continuing critical waivers, and workforce provisions.
Specifically, the legislation would:
-
Prevent the 4% Statutory Pay-As-You-Go (PAYGO) sequester for two years;
-
Extend for two years critical rural Medicare programs, telehealth flexibilities, and the Acute Hospital Care at Home;
-
Reduce the physician fee schedule cut from 4.5% to 2% for 2023 and approximately 3% for 2024;
-
Provide 200 additional Medicare-funded graduate medical education positions, half of which would be dedicated to psychiatry and psychiatry subspecialty residencies;
-
Take several steps to improve access to behavioral health services; and
-
Make improvements to the government's ability to prepare for future emergencies.
IHA Take
While the suspension of the sequester and extending the Medicare-Dependent Hospital (MDH) program and Low-Volume Hospital Adjustment (LVA) programs were critical wins, there are some disappointments.
The legislation does not include a Medicaid Disproportionate Share Hospital (DSH) “fix" supported by the IHA, other state hospital associations, and safety net hospitals. Without this language, Medicare-Medicaid dual eligible costs will no longer be included in the Hospital Specific Limits under the Medicaid DSH program. We believe Congress erred when this change was made in 2020, and IHA will continue to advocate for regulatory and legislative relief.
In addition, the omnibus does not fully reverse the looming Medicare physician fee schedule cuts. This is particularly painful in Indiana, where numerous studies show that physicians' reimbursement from commercial insurers is near the lowest in the country. If Medicare continues to underfund doctors, this will only serve to increase Indiana's already massive financial burden of subsidies. Without hospitals supporting physicians through these subsidies and employment, access for Hoosiers would be decimated. We must advocate for these cuts to be reversed. Please let your US Senators and your member of Congress know that these items are issues that we need them to address as early as possible in 2023.
Legislative Update - November 28, 2022
 Hospital Leaders Gather at Statehouse for Organization Day
Hospital Leaders Gather at Statehouse for Organization Day
IHA members from across the state gathered at the Indiana Statehouse last week to observe Organization Day and meet with legislators. On Organization Day, the legislature reconvenes to swear in new legislators, and legislative leadership discusses essential goals for the upcoming session.
IHA members met with individual legislators to share hospital accomplishments and policy priorities, had lunch discussions with legislators across the state on various healthcare issues, and viewed the session. In addition, IHA Board Chair Brad Smith, Public Health Committee Chair Dr. Brad Barrett, and IHA President Brian Tabor spoke to the group, sharing information about IHA and the legislative process for health policy.
The proactive nature of this gathering allowed hospital leaders to connect with legislators and advocate for their hospitals in advance of any legislative challenges that may arise in the 2023 session. IHA is grateful to the members who could attend the event last week and to all of our members who continue to advocate for their hospitals in the local community. There is no substitute for face-to-face conversations, and your representation of Indiana hospitals will continue to produce benefits in the coming months.
If you would like assistance connecting with your local legislators to share about your hospital’s impact on your community, please reach out to IHA’s Government Relations Team. We would be glad to help.
 New Pharmacy Benefit Managers Rules Adopted
New Pharmacy Benefit Managers Rules Adopted
The Indiana Department of Insurance (IDOI) recently adopted rules governing the licensure of Pharmacy Benefit Managers (PBM). In 2020, the Indiana General Assembly passed Senate Enrolled Act (SEA) 241, authored by State Senator Liz Brown (R-Fort Wayne), which required PBMs to be licensed to do business in the state. In addition, the law required IDOI to adopt rules to implement and enforce the new licensure requirements effectively. The newly adopted rules are part of policymakers’ increasing interest in the PBM industry in Indiana and across the country. As many states have prioritized health care cost transparency for consumers, Indiana lawmakers will likely continue to address the need to shed light on this evolving industry and its impact on the cost of health care. You can
read the PBM rules here.
Legislative Update - October 24, 2022
 Lawmakers Focus on Health Care Markets
Lawmakers Focus on Health Care Markets
A joint meeting was held on Thursday, October 20th, between the Interim Study Committee on Financial Institutions and the Interim Study Committee on Public Health, Behavioral Health, and Human Services. During the meeting, the groups reviewed and discussed two market concentration reports reviewing various stakeholders in the health care industry.
The market concentration reports were required by House Enrolled Act (HEA) 1405, passed during the 2021 legislative session. HEA 1405 directed the Legislative Services Agency (LSA) to commission a study on market concentration for health care-related industries such as hospitals, insurers, physicians, Pharmacy Benefit Managers (PBM), and retail pharmacies. The joint committee received presentations from the organizations selected by LSA to conduct the studies.
The Petris Center for Health Care Markets and Consumer Welfare, within the University of California Berkeley’s School of Public Health, was selected to report on insurer, hospital, and physician markets. In addition, Indiana University’s School of Public and Environmental Affairs was chosen to analyze pharmacy-related industries. The committee allowed public testimony and heard from the sectors represented in both reports.

Brian Tabor, IHA President (pictured right), testified on Indiana’s competitive landscape between health care systems across the state by providing recent examples that were omitted from the reports. He also emphasized Hoosiers’ poor health metrics and hospitals’ commitment to affordability, as evidenced by the progress on price transparency. Tabor also reiterated IHA’s support for transparency beyond health care providers to improve the state’s overall health care costs.
Craig Kinyon, President, and CEO of Reid Health (main photo), shared with the committee the timely story of Reid’s commitment to building a new facility in Connersville. The groundbreaking for Reid Health Connersville was held the evening before the committee. We are genuinely grateful for Reid’s significant commitment to its communities and for Kinyon taking the time to share Reid's story.
 Dr. Paul Wong, Director of NERA Economic Consulting (pictured left), shared his analysis of the reports and identified issues with the information from a technical and economic perspective. He told the committee that the studies should be received with caution, as they did not include all of the necessary data to take any regulatory action.
Dr. Paul Wong, Director of NERA Economic Consulting (pictured left), shared his analysis of the reports and identified issues with the information from a technical and economic perspective. He told the committee that the studies should be received with caution, as they did not include all of the necessary data to take any regulatory action.
The committee reviewed the reports and took testimony but did not officially act on the information. Here you can find the Petris Center report and the IU report. In addition, click here to read IHA's letter to the committee and view the committee member handout.
Legislative Update - October 7, 2022
 Legislative Study Committees Discuss Health Care Topics
Legislative Study Committees Discuss Health Care Topics
Each year, the legislature spends part of the summer and fall conducting Interim Study Committees on various topics. The committee's goal is to hear expert testimony and provide the legislature with an improved understanding of complex topics before formulating legislation addressing the issues.
This week, IHA provided testimony in the Interim Study Committee on Financial Institutions and Insurance on prior authorization, and in the Interim Study Committee on Public Health, Behavioral Health, and Human Serviceson maternal mortality

Julie Slinker of Rush Memorial Hospital testified on prior authorization, representing IHA's positions on the issue. She shared the challenges and costs associated with the current prior authorization process. In addition, she made recommendations to the committee regarding some alternative approaches that may alleviate the burden prior authorization causes for providers. The recommendations included creating a pilot program to remove prior authorization requirements for a number of the most-approved CPT codes to determine whether reduced prior authorization requirements would alleviate cost and complication in care provision. IHA is grateful to Julie and Rush Memorial for providing expertise on this issue.
 Brittany Waggoner, IHA's Maternal and Infant Quality Improvement Advisor, provided testimony about maternal mortality in Indiana. The committee heard testimony about Indiana's most recently released Maternal Mortality Review Committee Report on maternal mortality. Brittany provided subsequent testimony explaining steps the state should take to improve Indiana's maternal mortality statistics. Brittany explained that maternal health is a public health issue, and by addressing public health issues across the state through funding and program support, the legislature will be helping improve the state's maternal health as well.
Brittany Waggoner, IHA's Maternal and Infant Quality Improvement Advisor, provided testimony about maternal mortality in Indiana. The committee heard testimony about Indiana's most recently released Maternal Mortality Review Committee Report on maternal mortality. Brittany provided subsequent testimony explaining steps the state should take to improve Indiana's maternal mortality statistics. Brittany explained that maternal health is a public health issue, and by addressing public health issues across the state through funding and program support, the legislature will be helping improve the state's maternal health as well.
The legislature will hold a joint meeting of these two study committees on October 20th to review a legislatively commissioned study on market concentration of the health insurance industry, hospital industry, and other health-related industries in Indiana. IHA will provide testimony at this hearing and send an update about what takes place at the meeting.
 Indiana Behavioral Health Commission Releases Final Report
Indiana Behavioral Health Commission Releases Final Report
The Indiana Behavioral Health Commission released its final report last week. The statewide commission, comprised of elected officials, behavioral health providers, and other stakeholders, examined Indiana's behavioral health delivery system during the previous two years. The report is the culmination of that study, and contains recommendations for Indiana's mental health infrastructure, workforce issues, and other areas of interest, as well as funding recommendations.
The report contains recommendations specifically for the General Assembly to pass legislation requiring the Family and Social Services Administration (FSSA) to authorize EMS reimbursement for transport to behavioral health facilities. The change would allow individuals in a behavioral health crisis to be taken to the facility best suited to address their needs and, in turn, improve outcomes for these individuals.
The full report can be viewed on FSSA's website. IHA expects to see legislation in the 2023 session of the General Assembly in response to the recommendations in the report and will continue to provide information on those developments as they occur. Our government relations team welcomes any feedback on those recommendations and related legislation.
 Senator Braun Co-Authors Letter About Drug Manufacturers
Senator Braun Co-Authors Letter About Drug Manufacturers
Last week, Senator Mike Braun (R-IN) and Senator Joe Manchin (D-WV) sent a letter to U.S. Department of Health and Human Services (HHS) Secretary Xavier Becerra asking HHS to hold pharmaceutical companies accountable for their continued violations of the 340B Drug Pricing Program.
They asked HHS to "take immediate action to stop a series of alarming and escalating actions taken by several of the largest U.S. drug manufacturers and other stakeholders against our safety-net providers who participate in the 340B drug pricing program. These actions are causing significant harm to safety-net providers participating in the 340B program…."
IHA president Brian Tabor thanked both senators for their attention on this issue. Tabor said, "Our members are grateful to Senator Braun and Senator Manchin for leading in support of health care providers in Indiana and West Virginia, as well as those across the country on this urgent issue. The 340B drug pricing program is critical for hospitals and other entities that serve low-income patients. Given the current financial difficulties that our members are facing, further erosion of the 340B program threatens access to care in communities across Indiana."
The full letter can be found here.
Legislative Update - September 23, 2022
 Owen County Judge Issues Preliminary Injunction Pausing Indiana's Abortion Ban
Owen County Judge Issues Preliminary Injunction Pausing Indiana's Abortion Ban
On Sept. 22, Judge Kelsey Blake Hanlon
issued a preliminary injunction to temporarily pause the implementation of
Senate Enrolled Act (SEA) 1.
Although the order applies statewide through the Medical Licensing Board, meaning licensure actions will be reviewed under the previous abortion framework, a conservative reading of the order only enjoins the seven county prosecutors who are named as defendants in the lawsuit from enforcing SEA 1. The seven county prosecutors specifically named as defendants in the lawsuit are the prosecutors of Hendricks, Lake, Marion, Monroe, St. Joseph, Tippecanoe, and Warrick Counties; leaving the remainder of the state's county prosecutors able to bring criminal charges for unlawful abortions under the framework of SEA 1. In addition, IHA is confirming whether the Indiana Department of Health (IDOH) will continue to license and inspect abortion clinics due to the preliminary injunction.
Judge Hanlon, an Owen County Judge, was appointed to the case
filed in the Monroe County Circuit Court on Aug. 30 after the two elected judges in Monroe County recused themselves.
Although Judge Hanlon previously denied a Motion for a Temporary Restraining Order, Judge Hanlon granted the preliminary injunction, finding the following:
The plaintiffs, including Planned Parenthood Northwest, is reasonably likely to prevail on the merits of the case, finding bodily autonomy has been recognized in Indiana case law as a basic component of liberty, and Indiana's Constitution guarantees the right to liberty under Article I, Section 1. The court found SEA 1 materially burdens the right to bodily autonomy "by making that autonomy largely contingent upon first experiencing extreme sexual violence or significant loss of physical health or death" and by "significantly and arbitrarily limiting…access to care" by limiting treatment to hospitals and ambulatory surgical centers (ASC) that are majority owned by hospitals.
The remedy at law is inadequate, and the plaintiffs will suffer irreparable harm pending resolution of the case, as a violation of the Indiana Constitution is irreparable harm for purposes of a preliminary injunction analysis, in and of itself.
The threatened injury to the plaintiffs outweighs the threatened harm if the preliminary injunction were denied.
The public interest will not be served if the preliminary injunction is not granted, because the public has an interest in constitutional rights being upheld, specifically finding that "the public has an interest in Hoosiers being able to make deeply private and personal decisions without undue governmental intrusion." While there is also a legitimate public interest served by protecting fetal life, the court found Indiana's previous abortion regulation regime is sufficient to protect fetal life until the permanent injunction is considered.
It is important to note that the court found the plaintiffs were not likely to prevail on their argument that SEA 1 violates the Indiana Constitution's Equal Privileges and Immunities Clause under Article I, Section 23, because there are rational reasons for ending the regime of licensing and inspecting abortion clinics, which burdens IDOH.
Additionally, a
third legal challenge to SEA 1 was filed this week. The case, The Satanic Temple v. Eric Holcomb and Todd Rokita was filed in federal court and raised alleged violations of the U.S. Constitution.
Since the release of the order, the Attorney General has announced that his office plans to appeal the order. Therefore, we expect several updates on SEA 1 in the coming weeks. While IHA cannot provide legal advice, please do not hesitate to contact a team member with questions on this update. We also encourage you to continue to review the order and any policies and procedures with legal counsel.
Legislative Update - September 16, 2022
 Legislation to Streamline Prior Authorization Passes House
Legislation to Streamline Prior Authorization Passes House
In a voice vote, The U.S. House of Representatives passed the Improving Seniors' Timely Access to Care Act (H.R. 3173) on Wednesday. The bill would streamline prior authorization processes for Medicare Advantage plans. Congressman Larry Bucshon (R-Ind.) introduced the bill last year and continues championing the cause.
The bill's goal is to reduce the time spent obtaining prior authorizations, requiring insurance companies to establish an electronic program for managing the process and directing real-time decisions for a list of routinely approved services to be determined by HHS.
Additionally, the legislation requires insurance companies to report their prior authorization approval rates to the Centers for Medicare and Medicaid Services, allowing further tracking and understanding of prior authorization utilization and processes as they apply to Medicare Advantage Plans.
The bill will now need to be considered by the Senate. The companion form of the bill is S. 3018, introduced by Senator Roger Marshall (R-Kan.).
 Update on SEA 1 Litigation
Update on SEA 1 Litigation
Senate Enrolled Act (SEA) 1 officially went into effect yesterday, September 15, and the Monroe County Circuit Court has denied the American Civil Liberties Union (ACLU) of Indiana's request for a temporary restraining order on the law. The Monroe County Circuit Court will now consider the ACLU of Indiana's request for a preliminary injunction on September 19. Two elected Democratic judges from Monroe County declined to handle the case without stating a reasoning. Judge Kelsey Hanlon, a Republican from neighboring Owen County, accepted the appointment as special judge last week.
IHA will provide any relevant updates on the outcome of that hearing. However, there has been no change to the effectiveness of SEA 1; as such, hospitals and ambulatory outpatient surgical centers should continue ensuring compliance with SEA 1.
As a reminder, the ACLU of Indiana's lawsuit filed in the Monroe County Circuit Court contends SEA 1 violates the Indiana Constitution's:
-
Right to liberty under Article 1, Section 1, as it impairs patients from exercising their substantive due process right to privacy, which encompasses the right to abortion.
-
Equal Privileges and Immunities Clause under Article 1, Section 23, by treating abortion clinics differently from hospitals and ambulatory outpatient surgical centers as a result of SEA 1's elimination of abortion clinics.
-
Guarantee of due course of law under Article 1, Section 12 due to the vagueness of the health or life exception.
The Marion County Superior Court has taken no action to date on the ACLU of Indiana's separate lawsuit alleging violations of Indiana's Religious Freedom Restoration Act. IHA will also keep you updated with any relevant updates from the Marion County Superior Court.
 New Chair of House Ways and Means Committee Announced
New Chair of House Ways and Means Committee Announced
Today, Speaker of the House Todd Huston (R-Fishers) announced the new chair of the House Ways and Means Committee would be Rep. Jeff Thompson (R-Lizton). Rep. Thompson is replacing Rep. Tim Brown (R-Crawfordsville), who announced his retirement earlier this year.
Thompson has been a member of the Indiana House of Representatives since 1998. He spent over 30 years as a teacher at Danville Community High School and owns and continues running a hay and straw business. He graduated from Purdue University in 1978.
Thompson will continue to chair the Interim Study Committee on Pension Management Oversight and will now take over for Rep. Brown as chair of the Interim Study Committee on Fiscal Policy and State Budget Committee. More information can be found in the House Republican Caucus press release.
Legislative Update - September 9, 2022
 Second Legal Challenge Filed to Indiana Abortion Law
Second Legal Challenge Filed to Indiana Abortion Law
On Sept. 8, the American Civil Liberties Union (ACLU) of Indiana
filed its second lawsuit against
Senate Enrolled Act (SEA) 1 on behalf of Hoosier Jews for Choice and several anonymous individuals in Marion County Superior Court. The lawsuit argues SEA 1 violates Indiana's Religious Freedom Restoration Act (RFRA), which prohibits government action that substantially burdens a person's religious exercise, unless the burden is in furtherance of a compelling governmental interest and is the least restrictive means of furthering that interest.
The lawsuit argues that the plaintiffs have sincere religious beliefs that may direct them to obtain an abortion under circumstances prohibited by SEA 1, and they are individually harmed based on the new framework of SEA 1. The lawsuit requests SEA 1 to be preliminarily and permanently enjoined.
The ACLU of Indiana's lawsuit alleging a violation of RFRA is in addition to the
lawsuit filed on Aug. 30 in the Monroe County Circuit Court alleging violations of the Indiana Constitution, as reported last week.
Although the lawsuit has been filed, the Marion County Superior Court has taken no action. Therefore, hospitals and ambulatory outpatient surgical centers should continue to work towards ensuring compliance with SEA 1 starting Sept. 15 should any pregnancy terminations falling under the definition of "abortion" occur thereafter. Further, no action has been taken in the Monroe County Circuit Court to date.
IHA will keep members updated on both lawsuits. If you have any questions, please don't hesitate to get in touch with IHA's Deputy General Counsel,
Laura Brown.
Legislative Update - September 2, 2022
Indiana’s New Abortion Law Faces Legal Challenge
On Aug. 30, the American Civil Liberties Union of Indiana, on behalf of Planned Parenthood Northwest, encompassing Hawaii, Alaska, Indiana, and Kentucky, and four additional plaintiffs, filed a lawsuit in the Monroe County Circuit Court to preliminarily and permanently enjoin
Senate Enrolled Act (SEA) 1from going into effect. Their request is to maintain Indiana's current abortion framework rather than the framework of SEA 1, which is effective Sept. 15.
Although the lawsuit has been filed, the Monroe County Circuit Court has taken no action to date. Hospitals and ambulatory outpatient surgical centers should continue to work towards ensuring compliance with SEA 1 starting Sept. 15 should any pregnancy terminations falling under the definition of "abortion" occur thereafter. As a reminder, the term "abortion" for purposes of the SEA 1 framework means "the termination of human pregnancy with an intention other than to produce a live birth or to remove a dead fetus. The term includes abortions by surgical procedures and by abortion-inducing drugs" (See IC 16-18-2-1).
The lawsuit argues that SEA 1 violates Indiana's Constitution for the following reasons:
-
The lawsuit contends SEA 1 violates the Indiana Constitution's right to liberty under Article 1, Section 1, as it impairs patients from exercising their substantive due process right to privacy, which encompasses the right to abortion.
-
The lawsuit contends SEA 1 violates the Indiana Constitution's Equal Privileges and Immunities Clause under Article 1, Section 23 by treating abortion clinics differently from hospitals and ambulatory outpatient surgical centers as a result of SEA 1's elimination of abortion clinics.
-
The lawsuit contends SEA 1 violates the Indiana Constitution's guarantee of due course of law under Article 1, Section 12 due to the vagueness of the health or life exception.
IHA will keep members updated regarding the litigation but encourages members to continue to work towards ensuring compliance with SEA 1 starting Sept. 15.
Below, you find helpful SEA 1-related documents for download:
-
SEA 1 Framework Memorandum
-
SEA 1 Q&A Document
-
 Sample Abortion Certification Form
Sample Abortion Certification Form
Please note that the above documents do not constitute legal advice. If you have any questions, please don't hesitate to get in touch with IHA's Deputy General Counsel, Laura Brown.
Legislative Update - August 5, 2022
 SB 1 Passes House on Third Reading
SB 1 Passes House on Third Reading
This week, the Indiana House of Representatives took up
Senate Bill (SB) 1 in the House Committee on Courts and Criminal Code, during which Dr. Eric Fish, CEO of Schneck Medical Center and Chair of IHA’s Council on Government Relations, testified to ensure any legislation enacted considers the environment for Indiana’s health care professionals, before the bill moved to the full House for consideration.
On August 5, SB 1 passed on the House on 3rd Reading by a vote of 62-38, and under the bill, as it passed the House, Indiana’s new abortion framework would be as follows:
Lawful Abortions: Abortions would be permitted:
If a physician determines, based on reasonable medical judgment, that an “abortion is necessary to prevent any serious health risk to the pregnant woman or to save the pregnant woman’s life” at any point in the pregnancy. An exemption for “health” was not included in the Senate’s version of the bill, and IHA advocated for its inclusion as the bill moved to the House. The term “serious health risk” is defined as a condition that has complicated the mother's medical condition and necessitates an abortion to prevent death or a serious risk of substantial and irreversible physical impairment of a major bodily function.
For a lethal fetal anomaly, within the first 20 weeks. However, an abortion may still be provided for a lethal fetal anomaly if, after the first 20 weeks, the anomaly poses a serious health risk to the pregnant women.
If the pregnancy was the result of rape or incest and is provided within the first 10 weeks. An affidavit is no longer required, as was required under the Senate’s version of the bill. A physician must instead certify in writing the abortion is being performed at the woman's request because the pregnancy is the result of rape or incest.
Facilities: Abortions clinics would no longer be permitted in Indiana, and any abortion, including the provision of abortion-inducing drugs, would be required to be provided either in a hospital or an ambulatory outpatient surgical center that has a majority ownership by a hospital licensed in Indiana. Abortions after 20 weeks would be required to be performed in a hospital only.
IVF: The bill is clear that the proposed framework would not apply to in vitro fertilization.
Enforcement Framework: The proposed framework does not include new criminal penalties. However, it is still a Level 5 Felony under the current regulatory framework to provide an unlawful abortion, and under the House’s version of the bill, the Medical Licensing Board would revoke a physician’s license if he or she is found to have provided an unlawful abortion.
Effective Date: At the request of IHA, the effective date of the bill was moved to September 15, 2022, to allow for additional time for implementation.
Public Reports: The Indiana Department of Health would be required to compile its report outlining Indiana’s abortion statistics on a quarterly basis, rather than a yearly basis, and the Statewide Maternal Mortality Review Committee would be required to study how changes in the state’s abortion laws affect maternal mortality in Indiana
The language that would have provided the attorney general with concurrent jurisdiction with a prosecuting attorney who categorically refuses to enforce certain criminal laws was removed from the bill, and other amendments to further narrow the framework of the bill were defeated
SB 1 now returns to the Senate for consideration of whether the changes by the House will be accepted in order to send the bill to the Governor or whether further changes will be considered. Once the legislation is finalized, IHA will distribute a memorandum outlining the new framework, with more specific definitions and details included.
 Wrap-around Funding and Inflationary Relief Bill Passes House
Wrap-around Funding and Inflationary Relief Bill Passes House
SB 2, which allocated funding for maternal and child health wrap-around services, was changed significantly in the House this week with amendments in both the
Committee on Ways and Means and in the full House. The bill still allocates the $45 million in funding for wrap-around services targeted at helping mothers and children, but the House amendments also took the approach of specifying funding for existing programs. Rep. Tim Brown (R-Crawfordsville), who chairs the Committee on Ways and Means and sponsored SB 2 in the House, explained that the intent was to start by shoring up programs that have already been established, including $10M for the Nurse Family Partnership Program; $5.5M for the Safety PIN Grant Fund; $1M for Safe Haven Boxes; and $10M for the Child Care and Development Fund, and then return for the regular legislative session in January to discuss further opportunities. Brittany Waggoner, Maternal and Infant Quality Improvement Advisor for IHA, testified in support of the provisions in the legislation that would increase funding to support maternal and infant health in Indiana. The $45 million may be used for the following services:
-
Supporting the health of pregnant women, postpartum mothers, and infants;
-
Support pregnancy planning;
-
Support low-income families with children less than four years of age;
-
Increase the number of families served through the Child Care Development Fund;
-
Support Indiana foster and adoptive families;
-
Support prevention-based programming to help prevent children from entering the department of child services system;
-
Support funding for newborn safety devices (baby boxes); and
-
Funding for providers of maternal support services.
The committee further amended the bill by adding an automatic taxpayer refund to provide inflationary relief, which was also included in HB 1001. The amended SB 2 passed the House Ways and Means Committee unanimously and was then considered on second reading by the full House. SB 2 was further amended on second reading on Thursday to lower the automatic taxpayer refund amount to $200, rather than the original $225, due to the expanded number of Hoosiers eligible for the refund. The House approved the final SB 2 on Friday by a vote of 93-6 and returned it to the Senate for final consideration. The Senate voted Friday afternoon to concur on the House changes by a vote of 37-9, and the bill will now be sent to the Governor.
Legislative Update - July 29, 2022
 Indiana Special Session Update
Indiana Special Session Update
The Indiana General Assembly convened on July 25 for a special session to update Indiana's abortion framework in light of the U.S. Supreme Court's
Dobbs opinion, consider wraparound funding for pregnant women and children, and provide inflationary relief. Under the Governor's Proclamation authorizing a special session, the legislature must adjourn no later than August 14.
While both the House and Senate introduced their own versions of inflationary relief, the Senate was the only chamber to file legislation updating Indiana's abortion framework, Senate Bill (SB) 1, authored by Senator Sue Glick (R – LaGrange). After almost 8 hours of testimony and over 60 individuals testifying, none of whom testified in support of the bill, SB 1 passed out of the Senate Committee on Rules and Legislative Procedure on July 26 by a vote of 7-5. Details of the legislation as it passed out of committee are as follows:
-
Lawful Abortions: Under the proposed framework, abortions will be permitted when:
-
A physician determines, based on reasonable medical judgment, that “an abortion is necessary to prevent a substantial permanent impairment of the life of the pregnant woman," which could include circumstances beyond imminent death; or
-
The pregnancy was the result of rape or incest. The abortion must be provided within 12 weeks if the individuals is less than 16 years of age and within 8 weeks if the individuals is at least 16 years of age. The pregnant woman will be required to provide the physician with a signed affidavit, which shall be included in the woman's permanent health record; a charge or conviction of rape or incest is not required.
-
Lethal Fetal Anomalies: The current definition of “abortion" does not include producing a live birth or removing a dead fetus and would be updated to also not include pregnancies that are terminated where the fetus suffers an “irremediable medical condition that is incompatible with sustained life outside the womb, regardless of when the child is born." Accordingly, pregnancy terminations as a result of an ectopic pregnancy or lethal fetal anomaly would be permitted and not included in the definition of “abortion," but such pregnancy terminations must still be reported.
-
IVF: The definitions of “fetus" and “pregnancy" would be updated to ensure the framework does not impact in vitro fertilization.
-
Surgical Abortions: Surgical abortions would only be permitted to be provided in hospitals and ambulatory surgical centers (ASC) that are owned by hospitals moving forward, unless it is necessary to perform the abortion in another location due to a medical emergency.
-
Abortion Inducing Drugs: Abortion-inducing drugs could continue to be provided in hospitals, ASCs, and abortion clinics, and the current framework would be retained, whereby the first abortion-inducing drug must be taken in the presence of a physician.
-
Enforcement Framework: The proposed framework does not include new criminal penalties. However, it is still a Level 5 Felony under the current regulatory framework to provide an unlawful abortion.
On July 28, SB 1 was heard on 2nd Reading, an opportunity for any member of the Senate to offer an amendment on the bill, with 62 amendments ultimately being filed. The bill was amended to require the affidavit to be notarized and to allow the attorney general to have concurrent jurisdiction with a prosecuting attorney in the prosecution of a criminal law if the prosecuting attorney categorically refuses to enforce a law. An amendment was also adopted to require the Statewide Maternal Mortality Review Committee to study how changes in the state's abortion laws affect maternal mortality in Indiana. Although other amendments were offered, including those to narrow the framework of the bill, they were not adopted.
The bill will now be heard on 3rd Reading on July 30 for a full vote by the Senate, and we expect the bill to be taken up by the House next week for further consideration.
 Wraparound Funding for Pregnant Women and Children
Wraparound Funding for Pregnant Women and Children
The Senate also heard SB 2, authored by Senator Travis Holdman (R – Markle), this week, which provides wraparound funding for pregnant women and children. IHA's Maternal and Infant Quality Improvement Advisor, Brittany Waggoner, testified in support of the bill, which allocates $45 million to the Hoosier Families First Fund.
Under the legislation, the State Budget Agency would be permitted to distribute funds to the Indiana Department of Health, the Indiana Family and Social Services Agency (FSSA), the Indiana Department of Child Services (DCS), and the Indiana Department of Homeland Security for existing and new programs to address:
-
Funding to support the health of pregnant women, postpartum mothers, and infants;
-
Pregnancy planning, including addressing barriers to long-acting reversible contraception;
-
Needs of low-income families with children under 4 years old;
-
Increased access to child care;
-
Support for foster and adoptive care;
-
Programs to prevent children from entering the DCS system; and
-
Funding for Safe Haven baby boxes and more.
The bill passed on 3rd Reading on July 29 and is expected to be taken up by the House next week as well.
 Inflationary Relief
Inflationary Relief
The House advanced
House Bill (HB) 1001, authored by Representative Sharon Negele (R – Attica), this week, which is intended to provide inflationary relief through the issuance an additional automatic taxpayer refund of $225.
The bill also includes several other provisions, including:
-
Providing a sales tax exemption for children's diapers.
-
Increasing the exemption amount for a dependent child and adding an additional exemption for an adopted child.
-
Adding donated breast milk; noninvasive prenatal and routine carrier screening for all pregnant women at any time during pregnancy; and costs of labor and delivery to the list of supplies and services provided by Medicaid and the Healthy Indiana Plan.
-
Requiring FSSA to seek necessary approval from the federal Department of Health and Human Services to provide reimbursement for long-acting reversible contraception.
-
Allowing a local health department, health care provider, or other human services provider to request a Safety PIN grant to assist individuals in seeking contraceptives, unless the grant would be utilized for the distribution of contraceptives through school-run programs or to a minor without the consent of the minor's parent or guardian.
The bill passed on 3rd Reading on July 29 and will now go to the Senate for further consideration. IHA's Government Relations team will continue to engage legislators on these important bills and keep members updated.
Legislative Update - June 24, 2022
 Governor Calls Special Session of the Legislature
Governor Calls Special Session of the Legislature
This week, Governor Holcomb signed a proclamation calling the General Assembly to convene for a special session beginning on July 6, 2022, to act on his recently proposed plan to return $1 billion in state reserves to Indiana taxpayers. The full proclamation can be found here.
Outside of Indiana’s regular legislative sessions each year, which meet according to strict statutory deadlines, the Governor may call the legislature back into a special session to consider pressing issues. The legislature is not required to begin its special session precisely on July 6. Still, they have 40 days from the date identified in the Governor’s proclamation to conduct their business before adjourning.
While the legislature is in special session, they may consider other issues besides the topics requested by the Governor. In March, members of the House and Senate sent a joint letter to Governor Holcomb requesting that he call the legislature back for a special session to consider state laws related to abortion in anticipation of a Supreme Court decision on the topic. Given the Supreme Court’s decision released today on Dobbs v. Jackson Women’s Health Organization, which held that the Constitution does not confer a right to abortion and the authority to regulate abortion is returned to the individual states, it is expected that the General Assembly will also consider legislation related to abortion regulation as discussed in their letter.
It is not yet clear how the legislature will move forward on either the Governor’s inflation relief initiative or legislation in response to the Dobbs decision. IHA is in close contact with legislators and other decision-makers and will continue to provide updates as more information comes to light.
If you have specific questions, please reach out to IHA’s Government Relations Team:
Trent Fox, Vice President of Government Relations
Kristin Schwartz, Director of Advocacy and Federal Relations
Laura Brown, Deputy General Counsel
Legislative Update - June 17, 2022
 New Laws Going into Effect July 1
New Laws Going into Effect July 1
While the effective dates of legislation passed by the Indiana General Assembly vary, many new laws go into effect on July 1 of the year they were enacted. Below are highlights of bills going into effect on July 1, 2022, that impact Indiana hospitals. A memorandum summarizing all of the bills enacted during the 2022 legislative session that impact IHA's members can be found here.
Good Faith Estimates
House Enrolled Act (HEA) 1238 updated various provisions across the Indiana Code that address good faith estimates (GFE). These updates provide that if practitioners or facilities are in compliance with federal GFE law, then they are also in compliance with the requirements of Indiana Code. This eliminates any discrepancies between the two laws. IHA worked with our partners at Hall Render to update
IHA's No Surprises Act Toolkit to reflect the changes, and the updated model forms can be utilized starting July 1, 2022.
Hospital Protocols for Ambulance Services
HEA 1314 specifies that the hospital protocols for the admission, treatment, and care of patients with extended lengths of stay under IC 16-21-2-5(a)(4) must include that a patient's attending physician or the physician's designee must sign an order when the patient needs ambulance services other than emergency ambulance services. The order must state the level of ambulance service needed for the patient and the condition or diagnosis of the patient that makes the transportation of the patient by ambulance necessary.
Worker's Compensation
HEA 1153 provides that if, after the occurrence of a worker's compensation accident, compensation is paid for temporary disability, then the two-year limitation period to file an application for an adjustment of the claim begins to run on the last date for which the compensation was paid.
Starting January 1, 2023, HEA 1153 adds ambulatory outpatient surgical centers (ASC) to the definition of “medical service facility" for purposes of the worker's compensation reimbursement framework. Under this change, ASCs will be permitted to negotiate their reimbursement for worker's compensation claims and, if an amount is not otherwise negotiated, reimbursement will be two hundred percent (200%) of the amount that would be paid to the ASC on the same date for the same service or product under the ASC's Medicare reimbursement rate. Language that would have required that reimbursement could “not exceed" two hundred percent (200%) of Medicare for all medical service facilities, including hospitals, was removed from the bill during the legislative session.
Unlawful Practice of Medicine
Senate Enrolled Act (SEA) 239 provides, for purposes of the law prohibiting the unlawful practice of medicine or osteopathic medicine, that the practice of medicine or osteopathic medicine includes attaching the following identifying terms or words to an individual's name:
-
(A) "doctor of medicine"; (B) "M.D."; (C) "doctor of osteopathy"; (D) "D.O."; (E) "physician"; (F) "osteopath"; (G) "osteopathic medical physician"; (H) "surgeon"; (I) "physician and surgeon"; (J) "anesthesiologist"; (K) "cardiologist"; (L) "dermatologist"; (M) "endocrinologist"; (N) "gastroenterologist"; (O) "gynecologist"; (P) "hematologist"; (Q) "internist"; (R) "laryngologist"; (S) "nephrologist"; (T) "neurologist"; (U) "obstetrician"; (V) "oncologist"; (W) "ophthalmologist"; (X) "orthopedic surgeon"; (Y) "orthopedist"; (Z) "otologist"; (AA) "otolaryngologist"; (BB) "otorhinolaryngologist"; (CC) "pathologist"; (DD) "pediatrician"; (EE) "primary care physician"; (FF) "proctologist"; (GG) "psychiatrist"; (HH) "radiologist"; (II) "rheumatologist"; (JJ) "rhinologist"; (KK) "urologist"; (LL) "medical doctor"; (MM) "family practice physician"; or (NN) "physiatrist".
Under this law, any verbal or written statement cannot include one of the above terms or words attached to an individual's name if that individual is not licensed to practice medicine or osteopathic medicine.
Telehealth
SEA 284 adds the following practitioners to the list of individuals able to provide telehealth services:
 Governor Holcomb Announces Inflationary Relief Proposal
Governor Holcomb Announces Inflationary Relief Proposal
On June 9, Governor Holcomb announced an inflationary relief proposal to return $1 billion of state reserves to Hoosier taxpayers through an additional automatic taxpayer refund (ATR). This announcement follows a revenue report for the state's fiscal year that was higher than expected.
Under Governor Holcomb's proposal, each taxpayer would collect $225 in an ATR, in addition to the $125 ATR issued earlier this year.
Governor Holcomb plans to work with legislative leaders to call a special session before the end of June to consider implementing his proposal.
IHA's Government Relations Team will update membership when the special session is expected and if additional items will be considered during the special session. Legislative leaders have already asked to be called into a special session if Roe v. Wade is overturned by the U.S. Supreme Court, but the exact timing of the Court's opinion and that subsequent special session are unknown at this time.
Legislative Update - May 27, 2022
 Legislature Holds Technical Corrections Day, Overrides Veto
Legislature Holds Technical Corrections Day, Overrides Veto
The Indiana General Assembly met for Technical Corrections Day on Tuesday. Annually, the legislature meets for one day to make technical corrections to the legislation that passed during the immediately preceding session. These corrections include correcting misspellings or fixing other drafting errors. No substantive changes are made to the legislation, but any clerical errors that need to be resolved must still have the legislature’s oversight.
In addition to these technical changes, the House and Senate both voted to override the Governor’s veto of
House Enrolled Act (HEA) 1041, which addressed transgender individuals’ participation in school sports. The override passed with a vote of 67-28 in the House and a vote of 32-15 in the Senate. The bill will go into effect on July 1, 2022.
 Interim Study Committee Topics Assigned
Interim Study Committee Topics Assigned
The Indiana General Assembly’s Legislative Council also met on Technical Corrections Day to finalize the topics to be assigned to Interim Study Committees. Interim Study Committees, which are comprised of members of both the House and Senate, meet throughout the summer and fall to study the issues assigned to them. The work products of these committees often inform legislative proposals for the upcoming session that will begin in January. IHA’s Government Relations Team will be watching each of these Interim Study Committees closely and will continue to keep the membership updated on those topics impacting Indiana’s hospitals.
The Interim Study Committee topics assigned for the 2022 interim can be found
here, and highlights are as follows:
• Market Concentration Study: During the 2021 legislative session, the Indiana General Assembly enacted House Enrolled Act 1405, which required a legislative study on the market concentration of the health care industry, including health insurers, hospitals, health care practitioners, pharmaceutical retailers, pharmacy benefit managers, and pharmacy services administration organizations. These specific industries were identified by the legislature as having a role in the cost of health care. The study is due by December 31, 2022, but the topic has been specifically assigned to the Interim Study Committee on Public Health, Behavioral Health, and Human Services and the Interim Study Committee on Financial Institutions and Insurance for a joint review and we expect a final report to be discussed in the fall.
• Prior Authorization: The Interim Study Committee on Financial Institutions and Insurance was also assigned the topic of whether a health insurer should be required to exempt a health care provider from needing to receive prior authorization on a particular health care service if the health care provider has continuously received approval for the health care service for a determined number of months. The concept, commonly known as a “Gold Card” program, was originally included in Senate Bill (SB) 249 during the 2022 legislative session, which was supported by IHA. While SB 249 was not ultimately enacted, this Interim Study Committee will allow the discussion to continue.
• Maternal Mortality: In addition to the joint review of the market concentration study, the Interim Study Committee on Public Health, Behavioral Health, and Human Services have been tasked with studying the topic of maternal mortality.
• Logansport State Hospital: The Interim Study Committee on Public Health, Behavioral Health, and Human Services were also assigned the topic of reviewing Logansport State Hospital's operations and hospital statistics, including staffing and patient care. The Interim Study Committee has been tasked with determining whether any changes are necessary to improve the hospital's current system, including appropriate training for staff.
 IDOI Reviewing APCD RFP Responses
IDOI Reviewing APCD RFP Responses
During the 2021 legislative session, the Indiana General Assembly enacted House Enrolled Act 1402, requiring Indiana to establish an All-Payer Claims Database (APCD). Since the passage of the legislation, the APCD Advisory Council has convened, to which IHA President Brian Tabor was appointed, and a
Request for Proposal (RFP) and
Scope of Work has been issued to secure an administrator for the database. This is an important step in developing an effective and meaningful tool for Hoosiers seeking health care pricing and quality information.
RFP responses were due to the state by Apr. 4, 2022, and the Indiana Department of Insurance is currently reviewing the RFP responses that were submitted. IHA will continue to provide updates when an RFP is awarded, the APCD administrator is announced, and the next steps are determined.
Legislative Update - March 11, 2022
End of Session Report
 2022 Indiana Legislative Session is Adjourned
2022 Indiana Legislative Session is Adjourned
Indiana's 2022 Legislative Session adjourned sine die (until next year) at 12:30 a.m. on March 9th. Though filled with unexpected twists and turns, the IHA team is pleased with the outcomes of this session and the accomplishments achieved—including both the helpful legislation passed and the harmful bills avoided. The participation of IHA members and their willingness to have conversations with their local legislators was vital to ensuring the needs of hospitals were accurately represented. IHA sincerely thanks our members for their time and constant communication, not only with legislators but with the IHA government relations team as well.
Your advocacy made a meaningful impact.
In total, 849 bills were introduced during the 2022 session. The House introduced 432 bills, and the Senate introduced 417 bills. By the end of session, 95 Senate bills and 83 House bills passed. They are now making their way across the Governor's desk for his signature or veto.
If you have any questions, concerns, or additional feedback about any legislation, please contact Trent Fox, IHA's Vice President of Government Relations,
tfox@ihaconnect.org; or Kristin Schwartz, IHA's Director of Advocacy and Federal Relations, at
kschwartz@ihaconnect.org.
In-Depth Analysis
IHA's Deputy General Counsel, Laura Brown, has written an in-depth analysis on bills passed this year that are of greatest interest to IHA's members.
The memo can be accessed here. For questions or additional information, Laura Brown can be reached at
lbrown@ihaconnect.org.
 IHA Agenda Legislation
IHA Agenda Legislation
IHA identified a proactive agenda for the 2022 legislative session based on the feedback of members and direction of the Board. This legislative session resulted in multiple excellent achievements for Indiana hospitals that will have a beneficial impact on Indiana's health care landscape for years to come.
Supporting Indiana's Health Care Workforce
HB 1003: House Bill (HB) 1003, authored by Rep. Ethan Manning (R-Denver) and sponsored by Sen. Mark Messmer (R-Jasper), has been named the “Nursing Indiana Back to Health" bill. This legislation focuses on expanding the number of nurses in Indiana through increasing nursing program enrollment, expanding the number of clinical simulation hours, and increasing the allowed number of adjunct nurse educators for associate degree programs. The bill also codifies the temporary health care registry that was previously established in Governor Holcomb's executive order, as well as adding additional paths for foreign-educated nurses to become licensed in the state. While Nursing Indiana Back to Health is not a complete antidote to Indiana's nursing shortage, it is an important step towards a solution.
SB 5: Authored by Sen. Liz Brown (R-Fort Wayne) and sponsored by Rep. Ann Vermilion (R-Marion), Senate Bill (SB) 5 provides license reciprocity for health care professionals in Indiana. Currently, only a few health care professions have license reciprocity, meaning that if they are licensed in another state, they can quickly receive an Indiana license to practice without starting the licensure process over from scratch. By instating reciprocity for the rest of Indiana's health care professions, it will be much easier for health care providers from other states to move to Indiana and practice without sacrificing quality or safety. In a similar vein, the interstate medical licensure compact (SB 251) and the psychology inter-jurisdictional compact (SB 365) were also both passed this session. Compacts have a similar goal to license reciprocity: allowing members of the compact to practice in participating states, of which Indiana will now be one. Both reciprocity and compacts are additional steps toward alleviating the health care workforce shortage in Indiana.
Parity in Health Care Transparency
SB 249: To continue improving Indiana's health care costs through transparency, SB 249 would have required health insurance companies to provide additional cost information to the public, in line with the price transparency hospitals have already engaged in. One provision of the bill would have required health insurance companies to provide the reasoning behind premium increases over 5%, which would have helped individual Hoosiers and employers better understand the drivers of cost year over year. SB 249 passed the Senate unanimously, but the House Insurance Committee chairman declined to hear the bill. Although the bill did not pass this year, IHA will continue to work with industry stakeholders and the legislature to continue on the path toward greater transparency in an effort to lower Indiana's health care costs.
HB 1238: In addition to the transparency initiatives, SB 249 also included language that aligned Indiana law with federal good faith estimate (GFE) requirements, providing that a practitioner or facility satisfies the requirements of the Indiana Code requiring GFEs by complying with the existing federal law. Although SB 249 did not pass, the GFE provisions were added to HB 1238, which did become law. IHA is working with our partners at Hall Render to update the No Surprises Act toolkit to reflect the changes to Indiana law that will go into effect on July 1, 2022.
Patient Safety in Specialty Drug Administration
HB 1158: In response to the Indiana Department of Health's July report on the best practices of “white bagging" in specialty drug administration, IHA worked with other stakeholders to pass legislation this session that would implement those best practices. Due to the large number of bills filed, the controversy surrounding the topic of white bagging, and the lack of time this session to consider all the topics raised, the legislature chose not to consider white bagging specifically. Despite the fact that the language did not pass, IHA is working with the Indiana Department of Health and the Indiana Professional Licensing Agency to identify and implement non-legislative solutions to ensure patient safety is preserved in any situation in which white bagging would be implemented.
Health Care Legislation of Interest
Every year, the legislature files bills on a multitude of topics. Topics this year included education, tax, and fiscal issues, transportation, utilities, and many others. Because health care is a topic of high interest and concern to the legislature and to their constituents, many bills related to health care regulation, services, and delivery are filed each session. Below are included some of the bills related to health care that passed this session.
A full list of IHA's bills of interest can be found here.
SB 239: This bill addresses practitioner advertising and says that practitioners who misrepresent their training or professional qualifications or provide misleading information are subject to disciplinary sanctions. This bill originally included requirements for provider badging in health care facilities, but IHA was successful in having that language removed before the bill passed.
SB 284: This legislation made further changes to Indiana's telehealth laws, following up on changes made last year to expand the providers who could practice through telehealth. This bill adds multiple provider types to the law, including occupational therapist assistants, clinical fellows, students and graduates of certain professional programs, and others. The bill also allows behavior health analysts to provide telehealth services for the period until the Indiana Professional Licensing Agency has completed licensure implementation for that profession.
HB 1001: The final version of this legislation contains the provisions that Governor Holcomb indicated would be necessary to end the state's public health emergency declaration, including flexibility to continue the enhanced FMAP and SNAP benefits and to continue efficiently vaccinating Hoosiers five years of age and older. With the passage of the bill, Governor Holcomb officially
rescinded the public health emergency. Legislative leaders have publicly stated that the passage of HEA 1001 was to ensure the state's public health emergency, which was set to expire on March 4, was not renewed. The bill also contains language addressing businesses' employee vaccine mandates. This language has been changed significantly since the bill was originally considered last fall. Fortunately, IHA was successful in exempting health care facilities to which the CMS Interim Final Rule applies from the new vaccine mandate requirements under HEA 1001.
Since the state's public health emergency has ended, the COVID-19 liability protections for health care facilities that were contained in
House Enrolled Act (HEA) 1002 have expired. However, the broader COVID-19 civil liability protections contained in
Senate Enrolled Act (SEA) 1 are still in effect through December 31, 2024. Under SEA 1, a person is immune from civil tort liability for damages arising from COVID-19 on the premises owned or operated by the person; on any premises on which the person or an employee or agent of the person provided property or services to another person; or during an activity managed, organized, or sponsored by the person (See IC 34-30-32-6), except for instances of gross negligence or willful or wanton misconduct (See
IC 34-30-32-7). The phrase “arising from COVID-19" means an injury or harm caused by or resulting from the actual, alleged, or possible exposure to or contraction of COVID-19, or services, treatment, or other actions performed for COVID-19 (See
IC 34-30-32-2).
HB 1002: Although the underlying content of HB 1002 is various tax matters, this bill also contains the final version of legislation that was formerly in
SB 407 regarding long-term services and supports (LTSS). The final language in HB 1002 says that the Family and Social Services Administration (FSSA) may not enter a final contract that would implement risk-based managed care for LTSS before January 31, 2023.
HB 1112: Starting in July 2023, this legislation requires FSSA and managed care entities to reimburse an EMS provider organization that is a Medicaid provider at a rate comparable to federal Medicare reimbursement. It also requires FSSA to apply for an amendment to the Medicaid waiver on Medicaid reimbursement for a children's hospital bordering Indiana. This is to factor in any cost outlier case in a manner that results in the final reimbursement rate being comparable to the current Medicare reimbursement rate for the service provided by the children's hospital, or one hundred thirty percent (130%) of the Medicaid reimbursement rate for a service that does not have a Medicare reimbursement rate. The provisions concerning the children's hospital bordering Indiana expires on July 1, 2023. IHA is closely monitoring this and will continue working with partners at FSSA to ensure the membership's interests are communicated.
HB 1140: HB 1140 expands Medicaid eligibility for pregnant women in Indiana. The legislation increases Medicaid income eligibility requirements, removes the Medicaid limitation that only allowed coverage for pregnancy-related services, and allows FSSA to extend postpartum Medicaid coverage from the minimum 60-day coverage to up to 12 months of coverage, beginning on the last day of the pregnancy.
HB 1153: This bill addresses workers' compensation rehabilitation. The underlying bill increases the workers' compensation benefit amount by three percent over a four-year period starting July 1, 2023. The legislation also includes ambulatory surgery centers in the workers' compensation reimbursement structure. Originally, the bill included language that would have changed the standard worker's compensation reimbursement rate for hospitals from 200% of Medicare to an amount “not to exceed" 200% of Medicare. This “not to exceed" language was problematic due to the uncertainty it would create in the reimbursement structure, making the non-negotiated rate negotiable. IHA worked to have the “not to exceed" language removed from the bill, allowing the original wording of the statute to remain in place.
HB 1254: HB 1254 deals with newborn screening. The bill requires that, beginning July 1, 2022, only a disorder recommended by a perinatal genetics and genomics advisory committee with expertise in newborn screening may be added to the list of disorders for which newborns must be examined in Indiana.
HB 1255: This legislation, which was promoted by Indiana's Attorney General, Todd Rokita, allows health-related licensing boards to investigate and discipline individuals who no longer hold an active license if the violation in question occurred while they held, and acted under, the license. The Office of the Attorney General is the enforcement arm of the Professional Licensing Agency, which houses the state's occupational licensing boards and commissions. This measure clarified a licensing board's authority to ensure a licensee will not be able to surrender their license in lieu of discipline.
HB 1313: This bill requires that the Indiana Department of Health establish guidance and standards for health care providers for screening children for lead poisoning. The bill also contains requirements for health care providers who provide services to children less than six years old regarding blood lead screening.
 Concerning Legislation Avoided
Concerning Legislation Avoided
While the IHA team spends considerable time and effort supporting and advocating for legislation to become law that would be helpful to hospitals, significant effort is also expended to ensure legislation that would be harmful to hospitals does not pass. Below are included examples of bills that were filed for consideration this year, but through the advocacy efforts of IHA and additional stakeholders, did not become law.
SB 405: This bill would have required city and county hospitals to disclose individual salaries of hospital employees, as well as financial information related to ownership, operation and management of a nursing facility especially related to the UPL program. Given the importance of the privacy of this information and the recent ruling from the Public Access Counselor's office, which held that this information constituted trade secrets, IHA worked with county hospital members and other stakeholders to ensure this bill did not receive a hearing in committee. The bill did not progress through the legislature and thus did not become law.
HB 1270: The most concerning part of HB 1270 was the changes made to the annual public forums that are required of not-for-profit hospitals and insurers based in Indiana. IHA is proud to say the hospitals impacted by the public forum requirements passed during the 2021 legislative session not only complied with the law but also excelled in telling the great story of the positive impact each hospital has in their respective communities and on the patients they serve every day. IHA is pleased to report this legislation was not considered, and therefore did not become law.
HB 1295: HB 1295 introduced arbitration as the required means of resolving disputes concerning “buyout" provisions in physician non-compete agreements. This legislation was problematic because non-compete agreements serve a crucial role in protecting investments made by hospitals in recruiting and retaining Indiana's world-class providers. In 2020, the legislature enacted a law requiring “reasonable" buyout provisions to be included in such contracts. IHA successfully persuaded lawmakers to give the 2020 law more time to be applied before opening it up and risking unintended consequences. This bill passed through the House, but due to the advocacy of IHA, was not considered in the Senate and did not become law.
Legislative Update - March 4, 2022
Public Health Emergency Ends
 The final version of
House Bill (HB) 1001 passed the House yesterday by a vote of 79-9. The bill contains the provisions that Governor Holcomb indicated would need to allow him to end the state's public health emergency declaration, including flexibility to continue the enhanced FMAP and SNAP benefits and to continue efficiently vaccinating Hoosiers five years of age and older. With the passage of the bill, Governor Holcomb
officially rescinded the public health emergency on Thursday. Legislative leaders have publicly stated that the passage of HB 1001 was to ensure the state's public health emergency, which was set to expire on March 4, was not renewed.
The final version of
House Bill (HB) 1001 passed the House yesterday by a vote of 79-9. The bill contains the provisions that Governor Holcomb indicated would need to allow him to end the state's public health emergency declaration, including flexibility to continue the enhanced FMAP and SNAP benefits and to continue efficiently vaccinating Hoosiers five years of age and older. With the passage of the bill, Governor Holcomb
officially rescinded the public health emergency on Thursday. Legislative leaders have publicly stated that the passage of HB 1001 was to ensure the state's public health emergency, which was set to expire on March 4, was not renewed.
The bill also contains language addressing businesses' employee vaccine mandates. This language has been changed significantly since the bill was originally considered last fall, and notably, health care facilities to which the CMS Interim Final Rule applies are exempt from the bill. IHA will distribute an in-depth analysis on this legislation for IHA membership, as well as other bills of interest including those summarized below, following the conclusion of the legislative session.
Worker's Compensation Bill Amended
 Throughout the session, IHA has been working with legislators and stakeholders on
HB 1153, which addresses worker's compensation rehabilitation. The underlying bill increases the workers' compensation benefit amount by three percent over a four-year period starting July 1, 2023. An additional goal of the legislature was to include ambulatory surgery centers in the worker's compensation reimbursement structure. Up until this week, the bill also included language that would have changed the standard worker's compensation reimbursement rate for hospitals from 200% of Medicare to an amount “not to exceed" 200% of Medicare. This “not to exceed" language was problematic due to the uncertainty it would create in the reimbursement structure, making the non-negotiated rate negotiable, in addition to creating an unnecessary market for repricers.
Throughout the session, IHA has been working with legislators and stakeholders on
HB 1153, which addresses worker's compensation rehabilitation. The underlying bill increases the workers' compensation benefit amount by three percent over a four-year period starting July 1, 2023. An additional goal of the legislature was to include ambulatory surgery centers in the worker's compensation reimbursement structure. Up until this week, the bill also included language that would have changed the standard worker's compensation reimbursement rate for hospitals from 200% of Medicare to an amount “not to exceed" 200% of Medicare. This “not to exceed" language was problematic due to the uncertainty it would create in the reimbursement structure, making the non-negotiated rate negotiable, in addition to creating an unnecessary market for repricers.
IHA worked with legislators and additional stakeholders to have the “not to exceed" language removed from the bill in a Second Reading Amendment in the Senate on Monday. The bill then passed out of the Senate, and the House author of the legislation has chosen to concur, which will allow the changes to be accepted and the bill to be sent to the Governor for his signature or veto without further changes.
Conference Committees in Full Swing
 Multiple bills were changed through the Conference Committee process this week as well. For more information about the Conference Committee Process, please click
here.
Multiple bills were changed through the Conference Committee process this week as well. For more information about the Conference Committee Process, please click
here.
Notably, language was added to
HB 1238 that aligns Indiana's good faith estimate law with the federal No Surprises Act that is now in place. Indiana enacted its good faith estimate law before the federal law was finalized, which has led to discrepancies. This language in HB 1238 provides that compliance with the federal No Surprises Act ensures compliance with state law.
Senate Bill (SB) 284, which allows additional health care professionals to provide telehealth services under Indiana law, and
SB 239, which prohibits practitioners from advertising deceptive or misleading information, both went through conference committee so that technical corrections could be made to both bills, though the substance of the bills was not altered. SB 239 previously contained requirements requiring health care providers to wear specific badges, but that language was removed from the bill earlier in session and has not been added again.
Conference committees have also been scheduled for next week on additional bills. The IHA team is continuing to monitor these bills before session is expected to end next week.
Legislative Update - February 25, 2022
Conference Committees Begin Next Week
 As the Indiana General Assembly nears the end of the 2022 legislative session, conferences committees will begin, which allow the House and Senate to resolve any remaining differences on legislation. If a bill makes it through its second chamber without changes, the bill is sent straight to the Governor for consideration. If a bill is changed in the second chamber, however, a different process must be followed.
As the Indiana General Assembly nears the end of the 2022 legislative session, conferences committees will begin, which allow the House and Senate to resolve any remaining differences on legislation. If a bill makes it through its second chamber without changes, the bill is sent straight to the Governor for consideration. If a bill is changed in the second chamber, however, a different process must be followed.
If the author of the bill agrees with the changes made in the second chamber, the author may concur with those changes. The concurrence is voted on by the originating chamber, and after passage, the bill is sent to the Governor. If the author of the bill does not agree with the changes made in the other chamber, however, the author may dissent on the changes. In this case, the bill is sent to a conference committee. A conference committee is made up of four legislative conferees, two from the House and two from the Senate, appointed by leadership and usually representing each of the four caucuses and generally including both the author and sponsor of the bill. These conferees meet in committee to discuss the language of concern in the bill and come to a consensus. The resulting committee report is then sent to both chambers for a vote. If it passes, the agreed-upon version of the bill is sent to the Governor for his signature or veto.
House Bills Change Status in Senate
 House Bill (HB) 1295, which addressed physician non-compete agreements, was not heard in committee this week and will not advance this session.
HB 1153, addressing workers' compensation benefits, was considered by the Senate Appropriations Committee, and IHA continues to work toward an acceptable form of the bill.
House Bill (HB) 1295, which addressed physician non-compete agreements, was not heard in committee this week and will not advance this session.
HB 1153, addressing workers' compensation benefits, was considered by the Senate Appropriations Committee, and IHA continues to work toward an acceptable form of the bill.
HB 1295, which would require disputes about physician non-compete agreements to be resolved through arbitration even if a buyout amount was previously agreed upon, was scheduled to be considered in the Senate Committee on Health and Provider Services this week. The committee meeting was canceled, however, which means HB 1295 will not advance this session. The IHA government relations team worked extensively behind the scenes to help legislators understand our concern that the bill would interfere with good-faith contract agreements between physicians and their employers (including hospitals). The language is considered “dead," but IHA will continue to monitor to ensure the language is not added into a different bill during conference committee.
HB 1153, which contains language to increase the workers' compensation benefit as well as include ambulatory surgery centers in the workers' compensation reimbursement framework, was considered in the Senate Committee on Appropriations on Thursday. The current version of the bill also changes the standard workers' compensation reimbursement rate of 200 percent of Medicare to an amount “not to exceed" 200 percent of Medicare. IHA and other provider stakeholders have been working to remove the “not to exceed" language from the bill due to the instability it would introduce into the workers' compensation reimbursement framework. The expected results of the language include increased workers' compensation disputes and reduced provider participation. While the language was not removed in committee this week, it is expected to be removed in a second reading amendment next week in the Senate.
Insurance Transparency Bill Not Considered in House
 As we previously reported, Senate Bill (SB) 249, authored by Senator Liz Brown (R-Fort Wayne), passed through the Senate unanimously. In keeping with health care transparency measures implemented over the last several years for hospitals, this legislation required certain transparency measures of Indiana insurance companies. The main provision of the bill required insurance companies to provide employers with an explanation of premium increases above five percent, giving insight into the reasoning behind the employer's increased health care costs.
As we previously reported, Senate Bill (SB) 249, authored by Senator Liz Brown (R-Fort Wayne), passed through the Senate unanimously. In keeping with health care transparency measures implemented over the last several years for hospitals, this legislation required certain transparency measures of Indiana insurance companies. The main provision of the bill required insurance companies to provide employers with an explanation of premium increases above five percent, giving insight into the reasoning behind the employer's increased health care costs.
While the bill received broad support from the legislature, representatives of the insurance industry expressed opposition to the bill. The chairman of the House Committee on Financial Institutions and Insurance chose not to schedule the bill in committee, which prevented the bill from advancing further this year. Although the language is no longer being considered, IHA continues to engage with insurance stakeholders and employers to identify equitable solutions to Indiana's health care costs and how we can address configuration and other technical issues with insurers outside of the legislative process.
Additionally, SB 249 contained language that would align Indiana's Good Faith Estimate Law with federal law. IHA and other interested stakeholders are working with legislators to amend that language into another bill to ensure compliance with the federal law would ensure compliance with state law.
Legislative Update - February 18, 2022
Bills to End Public Health Emergency Pass Health Committees
 Earlier this week,
Senate Bill (SB) 3 passed out of the
House Committee on Public Health and will now be considered by the full House of Representatives. This legislation includes the items requested by Governor Holcomb in order to responsibly end the Public Health Emergency declaration. IHA would like to recognize Mike Schroyer, President of Baptist Health Floyd, who testified in support of SB 3 and explained to the committee that even though COVID will be around for the foreseeable future, it is important to make permanent some of the lessons we've already learned throughout the pandemic.
Earlier this week,
Senate Bill (SB) 3 passed out of the
House Committee on Public Health and will now be considered by the full House of Representatives. This legislation includes the items requested by Governor Holcomb in order to responsibly end the Public Health Emergency declaration. IHA would like to recognize Mike Schroyer, President of Baptist Health Floyd, who testified in support of SB 3 and explained to the committee that even though COVID will be around for the foreseeable future, it is important to make permanent some of the lessons we've already learned throughout the pandemic.
Mr. Schroyer also testified in support of an amendment to
House Bill (HB) 1001 in the
Senate Committee on Health and Provider Services. As has been discussed previously, HB 1001 included concerning requirements for employer vaccine mandates implemented by employers. Senator Messmer (R-Jasper) worked to ensure facilities that are under the CMS rule requiring certain vaccine policies will be exempt from the legislation going forward. IHA is grateful for the Senator's efforts to ensure hospitals and the state can avoid any unnecessary conflicts between state law and federal regulations. HB 1001 will now be sent to the full Senate for consideration. Both bills will likely end up being finalized in conference committees at the end of session with heavy involvement from legislative leadership.
IHA's Nursing Indiana Back to Health Bill Passes the Senate
 The Senate passed
House Bill (HB) 1003, IHA's "Nursing Indiana Back to Health" bill, on Thursday. The bill addresses Indiana's nurse shortage by expanding the nurse education pipeline in a number of ways. These include increasing the percentage of instructors at two-year institutions who can be adjunct versus full-time and increasing the percentage of clinical hours that can be obtained in a simulation facility, among other provisions. IHA has supported the bill throughout the process and is grateful to Representative Manning (R-Denver) and Senator Messmer (R-Jasper) for carrying the bill through the House and Senate. Multiple representatives from IHA member hospitals, including Community Health Network, Good Samaritan Hospital, and IU Health, have testified about the importance of the bill's provisions in both the House and Senate committees.
The Senate passed
House Bill (HB) 1003, IHA's "Nursing Indiana Back to Health" bill, on Thursday. The bill addresses Indiana's nurse shortage by expanding the nurse education pipeline in a number of ways. These include increasing the percentage of instructors at two-year institutions who can be adjunct versus full-time and increasing the percentage of clinical hours that can be obtained in a simulation facility, among other provisions. IHA has supported the bill throughout the process and is grateful to Representative Manning (R-Denver) and Senator Messmer (R-Jasper) for carrying the bill through the House and Senate. Multiple representatives from IHA member hospitals, including Community Health Network, Good Samaritan Hospital, and IU Health, have testified about the importance of the bill's provisions in both the House and Senate committees.
IHA President Brian Tabor and Ivy Tech Community College President Dr. Sue Ellspermann authored a joint op-ed this week in support of HB 1003, praising the legislation as a step forward in supporting Indiana's health care workforce. The op-ed can be read
here.
Now that the bill has passed both the House and the Senate, Rep. Manning and Sen. Messmer will confer on the changes the bill underwent throughout the legislative process. The bill will then be sent to Governor Holcomb for his consideration.
Long-Term Services and Supports Legislation Progresses
 The
House Committee on Public Health heard
Senate Bill (SB) 407 on Wednesday. As amended, the legislation would allow FSSA to either implement risk-based managed care for long-term services and supports (LTSS) or implement fee-for-service care coordination via Primary Care Case Management Entities or Medicaid Accountable Care Organizations. FSSA's
current plan is to transition LTSS to an insurance-based managed care model by 2024. If FSSA continues to move forward with transitioning LTSS to risk-based managed care, the State Budget Committee must review the Request for Proposal before it is issued.
The
House Committee on Public Health heard
Senate Bill (SB) 407 on Wednesday. As amended, the legislation would allow FSSA to either implement risk-based managed care for long-term services and supports (LTSS) or implement fee-for-service care coordination via Primary Care Case Management Entities or Medicaid Accountable Care Organizations. FSSA's
current plan is to transition LTSS to an insurance-based managed care model by 2024. If FSSA continues to move forward with transitioning LTSS to risk-based managed care, the State Budget Committee must review the Request for Proposal before it is issued.
Under the amended bill, one of the selected entities must be “provider-owned," meaning at least fifty-one percent of the ownership interest must be held by state-licensed health care providers that are enrolled in the Medicaid program. The bill also outlines multiple parameters for the transition, including specific requirements for provider agreement terminations, prior authorizations, network adequacy, and more. Additionally, the bill requires FSSA to continue to determine the reimbursement rates for LTSS providers. A previous version of the bill would have limited the transition to a ten-county pilot program, but that approach was removed from the bill.
New language was also added to the bill addressing staffing agencies. Specifically, the language allows employers and applicants to report staffing agency violations of state law to the Indiana Department of Revenue and the Attorney General for investigation by the Attorney General's Division of Consumer Protection. As amended, SB 407 passed out of committee by a vote of 9-0 and was reassigned to the
House Committee on Ways and Means.
Maternal & Child Health Bills Advance
 Bills addressing Indiana's maternal and child health have continued through the legislative process as well. One concerns childhood lead screening and another with postpartum Medicaid coverage.
Bills addressing Indiana's maternal and child health have continued through the legislative process as well. One concerns childhood lead screening and another with postpartum Medicaid coverage.
HB 1313 passed through the
Senate Committee on Health and Provider Services. The bill would require the Indiana Department of Health (IDOH) to establish standards and guidance for providers to screen Indiana children for lead poisoning. Additionally, the bill requires health care providers caring for children less than six years of age to take certain actions dealing with blood lead screening tests. The legislation will now be sent to the full Senate for consideration.
HB 1140 addresses Medicaid coverage for pregnant women, specifically addressing an extension of Medicaid coverage for women who are postpartum. The bill was previously passed out of the Senate Committee on Health and Provider Services and was then sent to the
Senate Committee on Appropriations due to the cost considerations associated with the legislation. The Appropriations Committee amended the bill this week from its original form that required Medicaid coverage for 12 months postpartum. The bill as amended requires FSSA to provide at least 60 days of postpartum coverage and not more than 12 months, allowing the agency to make specific coverage decisions. The bill passed through Appropriations and will now be considered by the full Senate.
Legislative Update - February 11, 2022
Health Care Bills Considered in Health Committees
This week marked the beginning of the second half of session, with House bills making their way through the process in the Senate, and Senate bills in the House.
The House and Senate Health Committees both met on Wednesday morning to discuss bills of interest to hospitals.
House Bill (HB) 1003, IHA's Nursing Indiana Back to Health bill, was considered in the
Senate Health and Provider Services Committee. The bill, which addresses Indiana's nurse shortage by expanding the nurse education pipeline in a number of ways, was discussed extensively. IHA supported the bill and multiple representatives from member hospitals, including Community Health Network, Good Samaritan Hospital, and IU Health, testified about the importance of the bill's provisions. The bill passed unanimously and will now be considered by the full Senate.
The
House Committee on Public Health considered multiple bills this week related to Indiana's health care workforce as well.
Senate Bill (SB) 5, which provides license reciprocity for health care professionals, passed committee unanimously.
SB 251, which would enter Indiana in the interstate medical licensure compact, and
SB 365, which establishes the psychology interjurisdictional compact, also passed unanimously. The authors and sponsors of the bills stated their intent is to improve Hoosier access to care by expanding the health care workforce in Indiana.
SB 284, which expands the health care professionals who can practice telehealth in Indiana, also passed unanimously in the House Public Health committee. The bill was amended in the committee to ensure that the current practice for case managers is not impacted.
Public Health Emergency Legislation Update
 The Governor issued a new
executive order on February 1 that extends Indiana's public health emergency until March 4, 2022. There has been continued discussion in the Statehouse regarding legislation to end the public health emergency. Both
SB 3 and
HB 1001 contain the legislative elements necessary for Indiana to continue receiving federal funding after the state's public health emergency comes to an end. However, it is not yet clear which bill will continue to move forward.
The Governor issued a new
executive order on February 1 that extends Indiana's public health emergency until March 4, 2022. There has been continued discussion in the Statehouse regarding legislation to end the public health emergency. Both
SB 3 and
HB 1001 contain the legislative elements necessary for Indiana to continue receiving federal funding after the state's public health emergency comes to an end. However, it is not yet clear which bill will continue to move forward.
SB 3 contains only the
provisions outlined by the Governor to continue funding, as well as language IHA, requested to continue the COVID-19 Temporary Health Care Provider Registry through the end of the federal public health emergency, which some hospitals have been using to augment staffing during the pandemic. HB 1001 contains similar language, while also limiting the ability of businesses to implement vaccine mandates, should they deem it necessary for health and safety. The business community continues to express concern about the mandate language in HB 1001, as does IHA due to the conflict between HB 1001 and the CMS Interim Final Rule regarding vaccination requirements for applicable health care facilities
It is expected that either HB 1001 and SB 3 will be considered in committee within the next couple of weeks, and IHA will remain engaged with stakeholders to ensure any conflicts are addressed.
Legislative Update - February 4, 2022
Overview of Session Timeline
 The legislative session can be broken into two halves. During the first half, bills are considered in their chamber of origin (either the House or the Senate). They are heard in committee, potentially amended on second reading, and then voted on by the full chamber on third reading. The halfway point of session is identified by the third-reading deadline occurring in each chamber. If a bill is not passed out of one chamber by this date, it is essentially “dead". After the halfway point, which is affectionately called “halftime", all remaining bills switch chambers. Senate bills are considered in the House, and House bills are considered in the Senate. These bills all go through the same process as before—committee, second reading, and third reading.
The legislative session can be broken into two halves. During the first half, bills are considered in their chamber of origin (either the House or the Senate). They are heard in committee, potentially amended on second reading, and then voted on by the full chamber on third reading. The halfway point of session is identified by the third-reading deadline occurring in each chamber. If a bill is not passed out of one chamber by this date, it is essentially “dead". After the halfway point, which is affectionately called “halftime", all remaining bills switch chambers. Senate bills are considered in the House, and House bills are considered in the Senate. These bills all go through the same process as before—committee, second reading, and third reading.
If a bill passes through both chambers with no changes, the bill can be sent straight to the Governor's desk for his consideration of either his signature or veto. If changes have been made in the opposite chamber, the bill author has the option to agree with the changes and file a concurrence, sending the bill to the Governor, or the author can file a dissent. In the case of a dissent, the bill is sent to conference committee, where a smaller committee of legislators debates the changes in the bill and either agrees to a final version to be sent to the Governor, or the bill dies and does not advance further.
In odd-numbered years, the legislature passes a biennial budget. This year, because no budget needs to be passed, the session is shorter. The legislature is only expected to meet for 10 weeks at the most, which gives them even less time to move bills through the entire process. Because of these circumstances, many bills do not survive until the end of session. For a visual of the remaining bills, you can visit the
General Assembly's website, where bills listed in blue are still in process, and those listed in gray are “dead".
IHA's Legislative Priorities Update
 At the beginning of session, IHA outlined priorities that would be the focus of our attention and support during session this year. At the halfway point, those pieces of legislation have already undergone extensive consideration and IHA will continue to support their progress.
At the beginning of session, IHA outlined priorities that would be the focus of our attention and support during session this year. At the halfway point, those pieces of legislation have already undergone extensive consideration and IHA will continue to support their progress.
Support for Indiana's Health Care Workforce
House Bill (HB) 1003, known as the Nursing Indiana Back to Health bill, was voted out of the House and the Senate will take up consideration of it when they reconvene next week. The bill has garnered bipartisan support in the legislature, as well as extensive engagement from the stakeholder community. Hospitals, educational institutions, and nurse representatives have worked hard together to identify opportunities to support the legislation. The bill's goal is to expand the pipeline for nursing students in Indiana to improve the state's health care workforce shortage over the long-term.
Senate Bill (SB) 5, establishing reciprocity for health care provider licensure, has also been well-received in the legislature. The bill received widespread support in the Senate from provider groups. A few health care professions have been removed from the bill due to the fact that they already have reciprocity or a compact in statute.
SB 251, which establishes the interstate medical licensure compact, has also received support in the Senate. The bill would allow physicians who meet the qualifications of the compact to be licensed in compact member states. The current versions of both bills have been sent to the House for further consideration.
Parity in Health Care Transparency
SB 249, which deals with health insurance transparency, passed the Senate unanimously this week. In the wake of multiple years of focus on hospital price transparency, this bill continues the transparency conversation by addressing insurance premium transparency. Though the bill received contentious feedback from some representatives of the insurance industry during the Senate committee hearings, many legislators expressed their appreciation for the continued attention to lowering health care costs that the bill represents. The bill has been sent to the House for further consideration.
As was noted last week, a
recent report authored by
Kaufman Strategic Advisors revealed new insights into Indiana's medical costs. Specifically, the analysis revealed that the insurance companies in Indiana raised premiums faster than the cost of claims, which resulted in higher profits for insurance companies instead of lower premium costs. SB 249 would require greater transparency related to insurance premiums, providing a fuller picture of the drivers behind health care costs for Hoosiers.
Patient Safety in Specialty Drug Administration
HB 1158 contained various language related to health care, including the language dealing with specialty drug administration, otherwise known as white bagging. As is often the case during the legislative session (especially a short session), legislators found that there was insufficient time to fully discuss some of the issues contained in the bill. Accordingly, the language related to specialty drug administration was removed from the bill during its consideration in committee, along with language dealing with some other topics.
Although the language is not currently in a bill for consideration, there remain multiple opportunities during the second half of session to request consideration of the language to protect patient safety. IHA will continue to advocate for white bagging language during this session and will provide more updates as they become available.
Legislative Update - January 28, 2022
 Health Insurance Transparency Legislation Moves Forward
Health Insurance Transparency Legislation Moves Forward
Senate Bill (SB) 249, authored by Senator Liz Brown (R-Fort Wayne), was voted out of the
Senate Committee on Health and Provider Services earlier this week. SB 249 is part of IHA's legislative agenda and continues the legislature's work to achieve greater transparency across the health care continuum. This will ensure that Hoosiers have better access to data on the various components of Indiana's health care costs.
Brian Tabor, IHA President, testified in committee about the need for such legislation and how it will shed light on the “black box" of how health insurance premiums are calculated. The bill requires that if the premium for a health insurance policy is expected to increase five percent (5%) or greater as compared to the previous year, the insurer must submit written justification for the premium increase to the Indiana Department of Insurance (IDOI) for review and approval. When proposing this concept to Senator Brown for legislation, IHA's overall goal was to ensure both employers and individual Hoosiers understand the specific reasons why their premiums are increasing greater than 5% in any given year and how much is derived from insurers administering self-insured plans—a significant market in Indiana. This data will equip employers, individual Hoosiers, and policymakers with a better understanding of the various drivers of health care costs. SB 249 will be considered by the entire Senate early next week.
 New Analysis: Indiana's Medical Costs in Line with Nearby States
New Analysis: Indiana's Medical Costs in Line with Nearby States
In his testimony on SB 249, IHA President Brian Tabor cited a recently released study that reveals new insights into Indiana's medical costs. The report, authored by
Kaufman Strategic Advisors, analyzed publicly available data on insurance premiums and claims costs for fully insured plans from 2015 through 2020 to understand the critical drivers of premium increases for Hoosier employers and consumers.
The analysis found that the growth rate in average premiums over the six-year period for the fully insured health plans in Indiana, Illinois, and Ohio rose at significantly faster rates than incurred medical claims, contributing to the profitability of fully insured health plans in those states. This information underscores the importance of SB 249 and the data it would provide to Hoosiers regarding the drivers of their health care costs.
The full report can be found here and the recent IHA press release on the topic can
be found here.
full report can be found here and the recent IHA press release on the topic can
be found here.
 Health-related Bills Continue Through Process
Health-related Bills Continue Through Process
As discussed in previous legislative updates, multiple health care-related bills have been making their way through the legislative process. Multiple bills advanced this week as the General Assembly nears the halfway mark of session, at which point all bills that have passed one chamber will be sent to the other for further consideration.
SB 284, which further expands telehealth providers, passed the full Senate this week and has been sent to the House, where it will be sponsored by Rep. Barrett (R-Richmond).
SB 239, dealing with health care provider identification and advertising, was amended in the
Senate Health and Provider Services Committee this week. The language requiring health care providers to display their professional designation on their work badges was removed from the bill. The remaining language prohibits providers from engaging in false advertising related to their professional services.
In the House,
House Bill (HB) 1153 that addresses workers compensation, and
HB 1295 dealing with physician non-compete agreements, passed the House this week. Both bills will be sent to the Senate for further consideration and potential amendments. IHA is working with legislators on both bills to make improvements that ensure the policy is amendable for hospitals and other stakeholders involved.
 Bills on Maternal and Child Health Advance
Bills on Maternal and Child Health Advance
Among the many bills being considered in the General Assembly this year, there are multiple supporting maternal and child health. The bills deal with Medicaid eligibility for pregnant women, newborn screening processes, and childhood lead screening. These bills were successfully voted through the process in the House and will now be sent to the Senate for further consideration.
HB 1140, authored by Rep. Vermilion (R-Marion), expands Medicaid eligibility for pregnant women. Specifically, the bill increases the income eligibility requirement for pregnant women to qualify for Medicaid. It also removes the Medicaid limitation on the type of medical assistance coverage pregnant women can receive—currently they are only allowed to receive pregnancy-related services. The bill also extends postpartum Medicaid coverage for pregnant women to 12 months from the current 60 days.
Authored by Rep. Barrett (R-Richmond),
HB 1254 addresses newborn screening requirements. Beginning July 1, 2022, the bill requires that disorders being added to the required newborn screening list must be recommended by a perinatal genetics and genomics advisory committee. This committee, which has expertise in newborn screening, will use protocols established by the Indiana Department of Health to recommend the addition or deletion of disorders to the required examination list. The goal of this legislation is to clarify the process for establishing the list of disorders that appear on the newborn screening, rather than the multiple avenues now in place.
Also authored by Rep. Barrett,
HB 1313 deals with screening children for lead poisoning. The bill requires the Indiana Department of Health to establish standards for health care providers regarding screening children for lead poisoning. The bill also includes some requirements for health care providers who screen children less than six years of age, directing that providers take certain actions regarding the blood lead screening test. The bill establishes these provider requirements between January 1, 2023, and December 31, 2026.
Legislative Update - January 21, 2022
 Health Committees Discuss Telehealth, Noncompetes
Health Committees Discuss Telehealth, Noncompetes
The House Committee on Public Health and the Senate Committee on Health and Provider Services both considered additional legislation this week that would impact hospitals.
In the Senate, Senate Bill (SB) 284, authored by Senator Charbonneau (R-Valparaiso), makes updates to Indiana's telehealth statute, building on the work done in 2021 to expand the types of providers able to utilize telehealth technology to care for patients. This bill, which passed committee unanimously, adds students of included health care professions to the list of individuals eligible to provide telehealth services. The bill also adds behavior analysts to the provider list. IHA testified in support of the legislation in committee and will continue to support the legislation as it moves forward.
House Bill (HB) 1295, authored by Representative Judy (R-Fort Wayne) was voted out of the House Public Health Committee this week. The bill would make some adjustments to the execution of physician non-compete agreements. The legislation provides that binding arbitration would be the required method of resolution if a physician and employer cannot agree on a reasonable purchase price for the buyout provision in a non-compete agreement. IHA has requested that the bill be amended to make binding arbitration an option available to disputing parties rather than the required method. IHA's Government Relations team will continue to work with legislators to achieve an agreeable outcome on the legislation.
 Long-Term Services and Supports Bill Heard in Committee
Long-Term Services and Supports Bill Heard in Committee
The Senate Committee on Health & Provider Services heard SB 407 on Wednesday, which would require FSSA to pursue a fee-for-service integrated care model program for individuals receiving long-term services and supports to ensure care coordination for those eligible Hoosiers. This model would replace FSSA's current plan to transition long-term services and supports to an insurance-based managed care model by 2024. Steve Long, CEO of Hancock Regional Hospital, testified on the bill to educate the committee about the potential impact the transition to insurance-based managed care would have on Indiana's nursing facilities and their partnerships with county and municipal hospitals. IHA continues to work with stakeholder partners and the administration to ensure an appropriate balance can be struck for a successful program that accomplishes the shared goals of all parties involved. SB 407 passed out of committee by a vote of 8-2 and was reassigned to the Senate Committee on Appropriations for further consideration due to the potential fiscal impact of the legislation.
 Workforce Bills Continue to Progress
Workforce Bills Continue to Progress
This week, HB 1003, authored by Representative Manning (R-Denver) passed the House by a vote of 91-2. The legislation supports the nursing workforce by streamlining education regulations and ensuring more students have the opportunity to study nursing in Indiana. The legislation will now be sent over to the Senate for consideration, where Senator Messmer (R-Jasper) will sponsor it through committee and Senate discussions.
SB 251, which would implement the interstate medical licensure compact in Indiana, was passed out of the Senate on Thursday. This bill is another opportunity to continue easing the health care workforce shortage in Indiana, allowing physicians to become licensed more quickly through the compact. The bill will now be sent to the House for consideration and sponsored by Representative Vermilion (R-Marion).
 Worker's Compensation Bill in Progress
Worker's Compensation Bill in Progress
HB 1153, which addresses worker's compensation, was voted out of the House Committee on Employment, Labor and Pensions this week. The bill originally added ambulatory surgery centers (ASCs), physician-owned hospital outpatient departments (HOPDs), and other physician-owned outpatient care facilities to the list of facilities in Indiana that are reimbursed at a negotiated rate of 200% of Medicare for worker's compensation services. While adding ASCs to the list had been discussed at length in previous years, the other additions had not been vetted and the implementation was complex and potentially detrimental to the other entities and their contracts. For this reason, IHA lobbied to remove the other facilities and only include ASCs in the bill. This change was made before the bill was voted out of committee. The bill still contains language that limits the worker's compensation negotiated rate, saying it is “not to exceed" 200% of Medicare. IHA is continuing to work with the bill author, Representative Lehman (R-Berne), and other legislators to remove this language from the bill and maintain the current method of determining reimbursement between providers and employers.
Legislative Update - January 14, 2022
Governor Holcomb Gives State of the State Addres s
s
On Tuesday, Governor Holcomb gave his State of the State address to the Indiana General Assembly focusing on the growth Indiana has experienced even during the pandemic. He also gave special attention to the important work Indiana's health care providers and public health experts continue to do across the state.
The Governor asked all Hoosiers to speak to their doctor and become vaccinated to reduce the number of COVID-related hospitalizations. He acknowledged the strain and exhaustion health care providers have experienced over the last two years of the pandemic and thanked them for their service:
“No words, salary, or earthly awards will ever be enough to repay you for the lives you've cared for and saved. The ultimate judge will be kind to you for living your love for your neighbor."
The
Governor also shared his priorities to support Hoosier mental health services, as well as public health initiatives. He specifically mentioned the Indiana Public Health Commission, of which IHA President Brian Tabor is a member. The Commission will produce a report this summer that will recommend appropriate actions to improve Indiana's public health system for the legislature's consideration during the 2023 legislative session.
In his speech, the Governor also discussed additional priorities to continue building Indiana's broadband capacity, supporting Indiana's already friendly business climate, and promoting public safety.
Governor Holcomb's full State of the State address can be accessed here.
 Nursing Indiana Back to Health Bill Passes House Committee
Nursing Indiana Back to Health Bill Passes House Committee
This Wednesday, the House Committee on Public Health approved House Bill (HB) 1003, termed the “Nursing Indiana Back to Health" bill. The bill provides flexibilities for nursing programs to expand the nurse workforce pipeline to address Indiana's ongoing workforce shortage. Multiple representatives of IHA testified in support of the bill, including Jean Putnam from Community Health Network, Rachel Spalding from Good Samaritan Hospital, and Jason Gilbert from Indiana University Health.
Specifically, the legislation allows for increased growth rates for Indiana nursing educational institutions, relieves some restrictions on the requirements for educators, and adjusts additional regulations to streamline the process for nursing students to enter and complete nursing programs.
The legislation also provides additional pathways for foreign-educated nurses to become licensed in Indiana, which will ensure nurses who want to practice in Indiana are able to do so as soon as possible. The bill also includes an extension of the health care workforce registry that was originally established under Governor Holcomb's public health emergency order. This extension will allow individuals on the registry to continue to serve through the end of the federal public health emergency.
IHA appreciates Representative Ethan Manning's (R-Denver) willingness to author this legislation. The Nursing Indiana Back to Health bill passed the committee unanimously and will now be considered by the entire House.
 Workforce Legislation Passes Senate Committee
Workforce Legislation Passes Senate Committee
The Senate Committee on Health and Provider Services considered multiple bills on Wednesday that would ease Indiana's health care workforce shortage as well. The committee also considered legislation that would ensure a measured approach to ending the state public health emergency.
Senate Bill (SB) 5, authored by Senator Liz Brown (R-Fort Wayne) creates license reciprocity for health care workers licensed in other states without the delay of the full Indiana licensure process. Senator Brown also authored SB 251, which would allow Indiana to enter the interstate medical licensure compact. IHA testified in support of both pieces of legislation, and the committee passed both bills unanimously.
The committee also passed SB 3, authored by Senator Ed Charbonneau (R-Valparaiso), unanimously. Carol Dozier, CEO of King's Daughter's Health, testified on behalf of IHA in support of the bill. The legislation puts provisions into statute that would allow the state to continue receiving federal funding that is tied to the public health emergency in the event that Indiana's public health emergency is ended. IHA appreciates the Senate's thoughtful approach to the potential end of the emergency declaration. The committee also amended the bill to include the emergency health care workforce registry. The registry's inclusion in multiple bills will increase the opportunity for the language to become law at the end of the legislative process.
The bills will now advance to the full Senate for consideration.
Legislative Update - January 7, 2022
 2022 Legislative Session
2022 Legislative Session
The 2022 legislative session of the Indiana General Assembly convened on January 4. House and Senate leaders released their respective legislative agendas this week, and bills are already making their way through the process. The IHA government relations team is working closely with legislators and stakeholders to effectively represent the interests of hospitals.
The Senate Republicans' agenda includes three priorities for the legislative session, as follows:
- Making more Hoosiers eligible for the automatic taxpayer refund;
- Providing school funding stability for quarantined students; and
- Responsibly ending Indiana's public health emergency.
Senator Charbonneau (R-Valparaiso) has filed Senate Bill (SB) 3 to address the responsible ending of the public health emergency, which currently includes the three items originally outlined by Governor Holcomb. IHA is working closely with the Senator to ensure needed provisions are included in the legislation so hospitals will not lose necessary flexibilities to address COVID-19 in the event that the public health emergency is ended.
The House Republicans' agenda includes four priorities for the legislative session, as follows:
- Legislating COVID-19 exemptions and ending Indiana's public health emergency;
- Reducing Indiana's income and business personal property tax rates;
- Addressing the state's health care workforce shortage by supporting Hoosier nurses; and
- Boosting local public safety efforts.
House Bill (HB) 1003, filed by Representative Manning (R-Denver) addresses the House Republican's efforts to support Hoosier nurses and grow the nurse workforce pipeline. IHA worked closely with Rep. Manning to develop this legislation, which has been titled “Nursing Indiana Back to Health".
In even-numbered years, the General Assembly has a “short session", which means no budget is considered and the legislature meets for only 10 weeks. Given the limited timeframe, business will be conducted quickly in the Statehouse. The IHA team is working diligently to keep you apprised of issues as they come up, and we are happy to answer questions or provide additional information as needed. Please do not hesitate to reach out to us.
 Update on HB 1001 COVID-19 Vaccination Language
Update on HB 1001 COVID-19 Vaccination Language
The House Committee on Employment, Labor and Pensions passed HB 1001 out of committee this week. The bill contains language that requires a business to allow certain exemptions for employees if the business chooses to require the COVID-19 vaccination as a condition of employment. The bill is expected to be considered by the full House next week.
The bill was considered by two committees in the General Assembly in November and December and the legislators heard a total of fourteen hours of testimony on the legislation. IHA provided testimony in both committees about hospital concerns regarding the inconsistencies between the bill and the pending CMS rule requiring vaccinations for health care workers and other federal regulations. IHA is continuing to engage with legislators on this issue and will provide relevant updates as they become available.
 IHA Legislative Agenda
IHA Legislative Agenda
Over the past year, the IHA government relations team has worked with the IHA membership to develop a 2022 legislative agenda that addresses the most pressing needs and concerns of Indiana hospitals. The agenda includes specialty drug administration (white bagging), health care workforce shortage initiatives (including Nursing Indiana Back to Health), and insurer transparency.
Patient Safety in Specialty Drug Administration
During
the 2021 legislative session, it became clear that new insurer policies regarding white bagging of specialty drugs were causing delayed care and harm to patients and continue to do so. IHA worked with the legislature to pass a bill that required the Indiana Department of Health to produce a report of specialty drug administration best practices. This year, IHA and Hoosiers for Safe Meds have worked with Representative Ed Clere (R-New Albany) to introduce HB 1158, which puts the resulting best practices into Indiana code. Specifically, the bill requires the Indiana Board of Pharmacy to adopt rules to establish safeguards for the practice of white bagging.
Support for Indiana's Health Care Workforce
Hospitals continue to struggle with a depleted and exhausted workforce, and one method of addressing that challenge is legislation that will increase the nurse workforce pipeline and make obtaining a license easier. IHA has developed a legislative package that includes HB 1003, known as Nursing Indiana Back to Health, which removes barriers to flexibility and allows nursing schools to add additional students to begin addressing Indiana's workforce needs. The package also includes SB 5
, authored by Senator Liz Brown (R-Fort Wayne), which grants license reciprocity to multiple health care professions in Indiana.
Parity in Health Care Transparency
Over the past few years, the Indiana legislature and the federal government have both passed legislation regarding hospital price transparency, and hospitals have gone above and beyond to provide information to patients regarding the cost of their care. However, hospital price transparency does not tell the whole story of the cost of health care. SB 249
, authored by Senator Liz Brown, brings transparency parity to the health insurance industry, requiring insurance companies to provide explanations of premium increases and transparency about the costs employers incur for health care. By aligning insurance transparency requirements with existing hospital transparency requirements, Indiana will be better able to understand and address health care costs in the state.
IHA's full legislative agenda can be found here.
 IHA Responds to Letter from Legislature
IHA Responds to Letter from Legislature
This week, Speaker Todd Huston (R-Fishers) and President Pro Tempore Rod Bray (R-Martinsville) released a statement and letter addressed to certain non-profit hospitals and insurance companies in Indiana. The letter discussed health care costs in Indiana and directed the recipients to develop a plan to lower hospital facility costs by 2025. The letter indicated the plan should be presented to the legislature by April 2022. They wrote, “Absent a viable plan, we will be left with no choice but to pursue legislation to statutorily reduce prices."
IHA has had conversations with both Speaker Huston and President Pro Tempore Bray and has expressed dismay at the letter's tone and implications, as well as to remind legislators about the work hospitals have done and continue to do to lower health care costs and provide quality care to Hoosiers.
IHA President Brian Tabor released a statement in response to the letter:
“Indiana hospitals remain committed to addressing health care affordability for Hoosiers. Hospitals have demonstrated this commitment even during the pandemic, with health systems working with insurers and collaborating directly with employers to lower costs for patients and businesses. Indiana's hospitals have also been recognized for leading the country in transparency. These initiatives are already proving to be effective.
Indiana hospitals are leaders in efforts to lower costs while improving the state's health. However, until all stakeholders are at the table, these efforts will always fall short. We must stop oversimplifying the causes and engage in honest, inclusive discussions without the threat of legislative rate-setting or appealing to outdated studies."
There is currently no legislation pending regarding statutory price reductions, and IHA will continue to engage in conversations with legislators to avoid harmful legislation that would hinder the good work hospitals are already doing regarding health care costs in Indiana. The IHA Board has also met with both Speaker Huston and Senator Bray regarding this matter.
The full letter from the General Assembly to Non-Profit Hospitals can be read here.
To keep up to date with all bill changes and updates in real-time, visit the IHA 2022 Legislative Bill Track.
Legislative Update - December 17, 2021
IHA President Brian Tabor Testifies on HB 1001 in Committee This Week
This week, theHouse Committee on Employment, Labor and Pensionsheld a hearing onHB 1001, which contains similar language to the proposed legislation heard in committee before Thanksgiving (you can read more about that committee hearing here).
HB 1001 contains provisions to ensure continued federal matching funds for Medicaid, continuation of enhanced benefits for SNAP, and the ability to efficiently vaccinate 5- to 11-year-olds, in the event that Governor Holcomb ends the public health emergency.
The bill also contains language regarding employers' ability to require COVID-19 vaccinations for their employees. This language is in conflict with Equal Employment Opportunity Commission guidance on federal exemptions and the CMS Interim Final Rule (IFR) which, though currently enjoined, would require hospitals to meet specific employee vaccination requirements to continue receiving Medicare and Medicaid reimbursement.
Given this language, IHA President Brian Tabor testified in committee to share concerns about the potential conflict between state and federal law that this bill would create, as well as explaining the difficult situation hospitals are facing regarding surging patients and lack of staffing.
The committee did not vote on the bill following the extensive testimony, and the legislature has indicated they will continue to consider the legislation between now and the beginning of session on January 4th, 2022. IHA will continue to engage legislators and other stakeholders on this issue to achieve the best outcome for Indiana hospitals.
 President Biden Signs Legislative Package Extending Relief from Medicare Sequestration
President Biden Signs Legislative Package Extending Relief from Medicare Sequestration
Last Friday, President Biden signed a legislative package into law that contains provisions that provide financial relief for healthcare providers. Prior to the passage of the bill, Medicare Sequestration, which would reduce federal spending on Medicare by 2%, was due to begin on January 1, 2022. With the passage of the legislation, Medicare sequestration was delayed until April 1, 2022, and then reduced to a 1% sequester through June 30, 2022. The package also included a provision to stop the 4% PAYGO sequester from going into effect in 2022.
While further discussions about the future of Medicare sequester are expected, this new law provides a reprieve for hospitals by eliminating immediate funding cuts at the beginning of 2022 while the pandemic continues to challenge hospital operations.
Legislative Update - November 24, 2021
Click here to read the November 24 Legislative Update.
Legislative Update - November 19, 2021
 Important: IHA Surprise Billing Toolkit
Important: IHA Surprise Billing Toolkit
With a variety of new federal and state requirements designed to address surprise medical bills, IHA worked in conjunction with Hall Render to compile a comprehensive toolkit to assist IHA members in responding to the evolving legislative and regulatory landscape addressing out-of-network reimbursement, balance billing protections, and good faith estimates. The toolkit includes template documents that can be adapted by hospitals to assist in complying with current state and federal requirements. Download the toolkit items below.
-
IHA Toolkit for Compliance with Surprise Billing Laws
-
Updated 12.28.21 Attachment A: Model Disclosure Notice Regarding Patient Protections Against Suprise Billing
-
Updated 12.28.21Attachment B: Standard Notice and Consent to Balance Billing
-
Attachment C: Model Notice Regarding Right to Receive a Good Faith Estimate
- Attachment D: Form for Good Faith Estimate for Health Care Items and Services
Organization Day Kicks off 2022 Legislative Session
On Tuesday, legislators gathered at the Statehouse for Organization Day, which ceremonially began the 2022 session of the Indiana General Assembly. On this day, newly added legislators are sworn in, and the respective caucuses in the House and Senate are able to meet together and plan for the upcoming session. This is also an opportunity for legislators to meet with lobbyists, stakeholders, and other members of the public to discuss legislative priorities for the upcoming year. The IHA Government Relations team had a full day of productive meetings with legislators to discuss various priorities and express the needs and goals of Indiana’s hospitals in the upcoming year.
Speaker of the House Todd Huston (R-Fishers) shared remarks during the day’s session, providing a preview of legislative priorities for 2022. These priorities included helping Hoosier communities grow, looking at ways to reduce health care costs, anti-abortion efforts, a parenting bill of rights related to education, and tax refunds, among other priorities.
 Governor Holcomb Identifies for End of COVID-19 Public Health Emergency
Governor Holcomb Identifies for End of COVID-19 Public Health Emergency
On the same day that the legislature met for Organization Day, Governor Holcomb released a statement identifying three changes the Indiana General Assembly would need to make to state law in order for him to end Indiana’s public health emergency, as follows:
• Continuation of the federal matching funds for Medicaid expenditures;
• Continuation of the enhanced benefits for those receiving federal food assistance; and
• Extending the ability to efficiently vaccinate 5- to 11-year-olds.
The Governor’s full statement can be found here.
Legislative leaders are now contemplating whether to convene briefly in December to consider these items for adoption.
 Take Action: Ask Federal Senators to Support Prior Authorization Reform Bill
Take Action: Ask Federal Senators to Support Prior Authorization Reform Bill
We have heard from IHA members, and in particular, our post-acute members, that widely varying Medicare Advantage prior authorization (PA) policies are creating a tremendous burden on hospitals. This burden adds cost to our health care system, frustrates patients and families, and leads to provider burnout. Given the current health care workforce crisis, we need the federal government to act. Legislation supported by the AHA was introduced last month by Sen. Roger Marshall (R-KS), and companion legislation in the US House of Representatives was supported by some of our Congressional delegation, including Rep. Bucshon, Rep. Pence, and Rep. Walorski. We want our US Senate offices to know how important this issue is. Please use this letter to contact Senator Young and Senator Braun and ask them to support this legislation. You may customize the message as needed to reflect how these PA policies impact your specific organization, staff, and patients.

Indiana Division of Mental Health and Addiction Funding Opportunity
Funds have been secured through the SAMHSA State GLS Youth Suicide Prevention Grant to facilitate the implementation of new or expand/continue family peer support programming in emergency room healthcare settings across Indiana. The purpose of this program is to provide peer support to family/loved ones of youth who are experiencing a mental health and/or suicidal crisis requiring emergency services. RFF proposals are due to DMHA by December 3, 2021. More information can be found here.
Legislative Update - October 8, 2021

Indiana's Redistricting Proposal Becomes Law
This week Governor Holcomb signed House Bill 1581 into law, which contains the legislature's redistricting plan based on the 2020 census results. Due to the delay in releasing the final 2020 census results, the redistricting maps could not be drawn during the normal legislative session, as is normally the case. Instead, the legislature recessed in the spring rather than their normal adjournment for the year, with the expectation of coming back for a session in the autumn to address redistricting. House members returned in mid-September to begin discussions and have committee meetings to pass the House version of the new maps, including the House, Senate, and Congressional districts. The Senate then returned to the Statehouse at the end of September to vote on the maps and make some additional changes for the Senate districts. The final vote took place on October 1, after which the bill containing the finalized districts was sent to the Governor for his signature.
View maps below:
- Senate map
- House maps
- Congressional districts maps
 IDOH Updates Newborn Screening Rule
IDOH Updates Newborn Screening Rule
The Indiana Department of Health issued an Emergency Rule, LSA Document #21-438(E), to add Adrenoleukodystrophy to the list of disorders for which newborns and infants must be screened. The Emergency Rule is effective as of September 29, 2021. The remainder of the list of disorders for which newborns and infants must be screened remains the same. The Emergency Rule also increases the newborn screening fee from $115 to $120 based on the updated cost of the program with the addition of Adrenoleukodystrophy. If you have any questions, please contact IHA's Deputy General Counsel Laura Brown.
 Federal Agencies Release Part II of No Surprises Act Regulations
Federal Agencies Release Part II of No Surprises Act Regulations
On Sept. 30, Federal agencies issued Part II in a series of regulations for implementation of the No Surprises Act. This interim final rule deals with the independent dispute resolution process, which allows providers and health plans to adjudicate outstanding reimbursement disputes. The Agencies have also created a website that focuses on general information about No Surprises Act provisions, and includes a federal portal where organizations can apply to be certified as independent dispute resolution entities, as well as for providers to participate in the federal dispute resolution process. The rule also provides more information about the good-faith cost estimates that providers are required to share with uninsured or self-pay patients for scheduled services. Additionally, Part II identifies a process for uninsured or self-pay patients and providers to utilize regarding these cost estimates. CMS has provided a summary of the proposed rule on their website.
 Interim Committee on Public Policy Releases Recommendations
Interim Committee on Public Policy Releases Recommendations
The Interim Committee on Public Policy released their Draft Final Report and Proposed Findings and Recommendations on Tuesday. The committee made multiple recommendations to the legislature regarding telehealth and licensure of various health care professionals. The committee recommends that Indiana maximize the use of health care compacts where possible, including enacting the Interstate Medical Licensing Compact. The committee also recommends that the General Assembly adopt universal reciprocity legislation for health care providers. Additionally, the committee recommends appropriating money to the Indiana Professional Licensing Agency to provide technological improvements to make management of reciprocity and compacts more straightforward. Regarding telehealth, the committee recommends that the legislature amend the state's telehealth laws to allow physical therapy assistants and all mental health and behavioral health professionals to use telehealth. These recommendations are sent to the legislature for consideration as future legislation.
The full report can be found here.
Legislative Update - October 1, 2021
 Governor Holcomb Extends Executive Orders on COVID-19
Governor Holcomb Extends Executive Orders on COVID-19
Governor Holcomb's Executive Orders (EO) 21-26 and 21-27 took effect today, October 1, 2021. The EOs extends the state's public health emergency for an additional 30 days due to the surge related to the Delta variant. EO 21-27 contains extends and adds multiple provisions aimed at providing flexibility and relief to the healthcare community:
-
Extends temporary licensure of health workers and students through the end of the year
-
Hospitals are directed to continue evidence-based criteria to ensure sufficient capacity and staffing, and should postpone non-emergency surgeries and procedures where necessary. The EO notes that hospitals should consult the best practice and recommendations of their medical associations and industries when making this assessment.
-
Hospitals are required to continue to report information to the Indiana Department of Health's EM Resource system, including diversion status, hours spend in diversion for emergency departments and critical care units, and other information related to coordination and resources.
-
The Indiana Department of Insurance is directed to request insurers extend prior authorization timeframes for open and approved authorizations, and waive clinical information requirements for prior authorization in the case of patient transfer and discharge to post-acute, home-based, and other appropriate placement.
-
Advanced Practice Registered Nurses are allowed to provide service at multiple locations as long as they have an existing collaborative agreement on file.
-
Extends licensure expirations for MD, DO, RN, APRN, and Midwives 30 days past the October 31st, 2021 deadline.
-
Governor Holcomb stressed in the EO that unvaccinated individuals are most at risk for serious illness, hospitalization, and death related to COVID-19, and 1,701 of 1,721 of new hospitalized COVID-19 patients were unvaccinated individuals. The Governor urged Hoosiers to be vaccinated to be protected against hospitalization and serious illness from COVID-19.
A full text of the EOs can be found here.
 Trent Fox, IHA Vice President of Government Relations, Sworn in as Attorney
Trent Fox, IHA Vice President of Government Relations, Sworn in as Attorney
Trent Fox, Vice President of Government Relations for the Indiana Hospital Association, was sworn in today as an attorney on Friday in Fort Wayne, Indiana to become a member of the Indiana Bar Association. Although attorneys may choose to participate in a State Bar Association swearing-in ceremony, Trent chose to have former State Representative Casey Cox (R-Fort Wayne) administer the oath of office in the Allen County Courthouse. While Trent was in law school, he served as Rep. Cox's legislative aide when Rep. Cox was a member of the General Assembly. Along with Trent’s family, Ben Miles, President of Health Plan Services and Chief Advocacy Officer at Parkview Health, and Beth Lock, Director of Governmental and Legislative Affairs at Parkview Health, also attended the ceremony (pictured below along with IHA Director of Advocacy & Federal Relations Kristin Schwartz). As members of Parkview Health’s government relations team, both have worked closely with Trent in his role at IHA. Trent serves as the lead legislative representative at the Indiana Statehouse for the association.
Prior to joining IHA, he served as Chief of Staff to the Indiana State Health Commissioner, Dr. Kristina Box. He has also served as Director of Communications and Legislative Affairs at the Indiana Professional Licensing Agency, where he worked closely with Indiana’s prescription drug monitoring program, health profession regulatory bodies, and served as spokesman for the agency’s 38 boards and commissions. His experience also includes serving as Deputy Director of Legislative Operations for the Indiana House of Representatives and as Legislative Assistant to Speaker of the House Brian Bosma. He received his law degree at Indiana University Robert H. McKinney School of Law and a Bachelor of Science in legal studies from Indiana State University. Please join IHA in congratulating Trent Fox on this impressive accomplishment.

Legislative Update - September 10, 2021
 Indiana Hospital Association Recognizes Outstanding Individuals in Health Care
Indiana Hospital Association Recognizes Outstanding Individuals in Health Care
The Indiana Hospital Association (IHA) honored multiple individuals this week at its Annual Meeting, which was held virtually this year. Among the awards presented was the John C. Render Award for Health Policy. The award was created in 2011 and is presented to individuals who have had a significant influence on health care policy affecting Indiana hospitals. Render has had an enormous impact on health care, having dedicated his career to improving the lives of Hoosiers by advocating and educating on behalf of IHA’s member hospitals.
This year’s recipient of the John C. Render Award for Health Policy was the former Secretary of the Family and Social Services Administration (FSSA), Dr. Jennifer Sullivan. Dr. Sullivan served as FSSA Secretary for over six years, making her the longest-serving secretary in the agency’s history. Her tenure in the position was marked by multiple achievements contributing to the health and wellbeing of Hoosiers.
Additional awards and recipients can be found inIHA’s press release.
 CMS to Require COVID-19 Vaccination of Staff at Medicare & Medicaid-Certified Facilities
CMS to Require COVID-19 Vaccination of Staff at Medicare & Medicaid-Certified Facilities
On September 9, 2021, the federal Centers for Medicare & Medicaid Services (CMS) announced
it will require COVID-19 vaccination of staff at all Medicare and Medicaid-certified facilities, including hospitals, ambulatory surgical centers, skilled nursing facilities, home health agencies, and dialysis facilities. CMS is expected to issue an Interim Final Rule with Comment Period in October 2021 to implement this requirement. IHA will continue to provide updates as more information becomes available.
The Interim Final Rule is expected to apply to 50,000 healthcare providers and over 17 million healthcare staff at Medicare and Medicaid-certified facilities across the country.
 Indiana Medicaid Issues Prior Authorization Bulletins
Indiana Medicaid Issues Prior Authorization Bulletins
In response to the continuing impact of the Delta variant and Governor Holcomb’s recent Executive Order 21-24 regarding prior authorizations (PA), the Indiana Health Coverage Programs (IHCP) has issued several Bulletins related to PAs, as follows:
-
IHCP temporarily reinstates revisions to PA process for acute care hospital non-elective inpatient admissions (BT202174): Effective for dates of service (DOS) on or after August 30, 2021, acute care hospitals will only be required to submit basic information on the Universal PA Form for non-elective admissions and inter-hospital transfers that are necessary to increase bed capacity. Acute care hospitals must submit the PA request within 72 hours of the member’s admission, and authorizations will be automatically approved for a period of 60 days unless fewer days are requested.
-
IHCP temporarily revises timeframes for certain PA approvals (BT202178): Effective September 1, 2021, existing PAs will automatically be extended for 180 days from the expiration date of the PA for non-emergent surgeries or procedures that are postponed to ensure sufficient COVID-19 response capabilities.
-
IHCP reinstates inpatient SUD and psychiatric admission policy changes (BT202179): Effective for DOS on or after September 8, 2021, providers will only be required to submit basic information using the most appropriate IHCP PA form for inpatient substance use disorder (SUD) and psychiatric admissions. Providers must submit the PA request within 72 hours of the member’s admission, and initial PAs for inpatient SUD and psychiatric admissions will include seven days.
-
PA changes temporarily reinstated for some DME/HME services and supplies (BT202180): Effective for DOS on or after September 8, 2021, IHCP is temporarily removing PA requirements for the DME/HME services and supplies outlined in the Bulletin.
-
IHCP reinstates temporary PA changes for managed care SNF admissions (BT202181): Effective for DOS on or after September 8, 2021, providers will only be required to submit basic information using the Universal PA Form for skilled nursing facility (SNF) admissions. Providers must submit the PA request within 72 hours of the member’s admission, and authorizations will be approved for a period of 14 days unless fewer days are requested or the member has less than 14 days remaining in their skilled nursing benefit limit.
-
IHCP temporarily reinstates PA policy for LTAC and AIR facility admissions (BT202182): Effective for DOS on or after September 8, 2021, providers will only be required to submit basic information using the Universal PA Form for long-term acute care (LTAC) and acute inpatient rehabilitation (AIR) facility admissions. Providers must submit the PA request within 72 hours of the member’s admission, and authorizations will be approved for a period of 14 days.
Controlled Substance Registration to Be Required for Ambulance Service Providers
On August 25, 2021, the Indiana Board of Pharmacy published LSA Document #20-455(F), a Final Rule requiring each ambulance service provider that purchases, stores, or dispenses any controlled substance to obtain a controlled substance registration (CSR). This Final Rule repeals the previous language under 856 IAC 2-3-4(c) that waived the requirement for ambulance service providers to obtain a CSR. The Final Rule is effective 30 days from its publication.
Further highlights from the Final Rule are as follows:
-
CSR Registration: A separate registration is required for each principal place of business where controlled substances are stored. However, a separate registration is not required for each ambulance owned or operated by the provider. Additionally, agents or employees of the provider are not required to register if they are acting in the usual course of employment.
-
Hospital Pharmacies: A hospital pharmacy may, but is not required to:
-
Enter into a written agreement with an ambulance service provider to provide, sell or deliver stocks of controlled substances for use in an ambulance; or
-
Enter into a written agreement with an ambulance service provider to act as an agent for the provider and supply a sub-stock of controlled substances for use in the provider's ambulances.
-
Hospital CSR: A registrant owned or operated by a hospital may:
-
Utilize the hospital pharmacy's registration for the delivery of controlled substances for use in any authorized ambulance;
-
Maintain the provider's controlled substances as part of the hospital's controlled substances sub-stock; and
-
Have the hospital act as the agent for the provider.
-
Note: a separate CSR is still needed by the ambulance service provider for other actions, such as purchasing and dispensing controlled substances.
We encourage you to review the entirety of the rule, which includes documentation, storage, and security requirements for registrants.
Legislative Update - September 3, 2021
Governor Holcomb Issues New Executive Order on COVID-19
Governor Holcomb's Executive Order (EO) 21-24 took effect on September 2, 2021. The EO extends the state's public health emergency due to the surge related to the Delta variant. The EO contains multiple provisions aimed at providing flexibility and relief to the healthcare community:
-
Hospitals are directed to implement evidence-based criteria to ensure sufficient capacity and staffing, and should postpone non-emergency surgeries and procedures where necessary. The EO notes that hospitals should consult the best practice and recommendations of their medical associations and industries when making this assessment.
-
Hospitals are required to report information to the Indiana Department of Health's EM Resource system, including diversion status, hours spend in diversion for emergency departments and critical care units, and other information related to coordination and resources.
-
The Indiana Department of Insurance is directed to request insurers extend prior authorization timeframes for open and approved authorizations, and waive clinical information requirements for prior authorization in the case of patient transfer and discharge to post-acute, home-based, and other appropriate placement.
-
Advanced Practice Registered Nurses are allowed to provide service at multiple locations as long as they have an existing collaborative agreement on file.
Governor Holcomb stressed in the EO that unvaccinated individuals are most at risk for serious illness, hospitalization, and death related to COVID-19, and 93% of new COVID-19 cases since January of this year were unvaccinated individuals. The Governor urged Hoosiers to be vaccinated to be protected against hospitalization and serious illness from COVID-19.
The full text of the EO can be foundhere.
IHA President Brian Tabor issued a statement on the EO: “We appreciate that the State of Indiana recognizes how strained Indiana hospitals currently are with the Delta variant wave. One region in southern Indiana has already exceeded its highest number of COVID-19 hospitalizations at any point during the pandemic. According to Kentucky Governor Andy Beshear, only 115 intensive care unit (ICU) beds
were available in the entire state of Kentucky earlier this week. There is a massive storm cloud of this virus sweeping up through Indiana, and increasing our state's vaccination rate is the most effective way to ease the burden on our courageous health care heroes and ensure a hospital bed for every Hoosier that needs one."

Interim Committee on Public Health Concludes and Releases Report
The Interim Committee on Public Health, Behavioral Health, and Human Services had their final meeting on Wednesday to discuss outstanding topics and to present their draft final report.
The committee heard testimony from the Alcohol and Tobacco Commission (ATC) regarding the implementation and enforcement of smoking laws. Additionally, Dr. Box testified on behalf of the Indiana Department of Health to provide an update to the General Assembly on the OB Navigator program, which is now known as My Healthy Baby. The presentation contained preliminary data, and IDOH plans to release expanded data from July 1, 2020 – June 30, 2021, in November. Through December 2020, over 1,200 women accepted referrals for home visiting services to receive care for their pregnancy. Dr. Box's full presentation can be viewed here.
here.
The committee also released their draft report containing the committee's findings and recommendations based on the meeting presentations. The purpose of the report is to direct and inform any potential legislation on the topics addressed. However, while legislation may be filed on these topics, the report recommendations do not automatically require legislation. The committee's recommendations include:
-
Multiple recommendations regarding the state's trauma care system, including urging the Indiana State Trauma Care Committee to assess Indiana's trauma center system
-
Multiple recommendations concerning Indiana's transition to risk-based or capitated managed care for long-term care Medicaid services, including urging FSSA to review and address the impact on intergovernmental transfers and to continue meeting with stakeholders regarding the transition.
The full draft report can be foundhere.
 IHA named to Governor’s Public Health Commission
IHA named to Governor’s Public Health Commission
On August 18th, Governor Holcomb issued an Executive Order (EO) establishing the Governor’s Public Health Commission. The goal of the commission is to advise the Governor and the Indiana Department of Health regarding Indiana’s public health system. Citing Indiana’s poor public health rankings nationally, as well as the challenges and lessons learned from the COVID-19 pandemic, the Governor’s EO states that Indiana’s public health system would benefit from comprehensive review and evaluation with the aim of improving efficiency and efficacy for Hoosier health. The EO names IHA as one of the 15 commission members, along with the State Health Commissioner, the Indiana Rural Health Association, the Indiana Minority Health Coalition, the Indiana Public Health Association, three elected officials, a representative for healthcare workforce initiative, an academician from the public health field, a public health administrator from the Local Health Department Manager’s Association, two local health officers, and two representatives of the public, who will serve as co-chairs of the commission
The EO creating the commission can be foundhere.
Legislative Update - August 13, 2021
 Interim Public Health Committee Discusses Long Term Care
Interim Public Health Committee Discusses Long Term Care
This week, the Interim Study Committee on Public Health, Behavioral Health, and Human Services met to discuss Long Term Care Services and Supports. The committee heard testimony from Dr. Dan Rusyniak, newly appointed FSSA Secretary, during which he outlined the state’s current path to LTSS reform, including discussions of risk-based managed care or capitated, managed care for Medicaid recipients. Of great concern is the goal to allow more Hoosiers to age in their homes while receiving any needed care if they so choose. Dr. Rusyniak emphasized FSSA’s focus on choice, cost, and quality of care, and their prioritization of stakeholder partnership and feedback during the ongoing reform process. Dr. Rusyniak’s presentation can be viewed
here. The committee received additional testimony from long-term care stakeholders, including the Indiana Health Care Association, LeadingAge, AARP, the Indiana Association of Area Agencies on Aging, and others.
Chairman Charbonneau confirmed that the committee will meet once more during the interim on August 25 to discuss further topics, and then will adopt the final study committee report with any recommendations the committee feels are necessary.
 Regulatory Waivers Renewed
Regulatory Waivers Renewed
The Indiana Department of Health reissued temporary blanket waivers for hospitals and ambulatory outpatient surgical centers on August 9th. The new order allows all previously issued waivers for acute and continuing care facilities to continue. These reissued waivers were effective on August 9, 2021, and will be in effect for 45 days past the expiration of the current Public Health Emergency declared by Governor Holcomb. You can find the notice of waivers here.
 Hospital Price Transparency Rule
Hospital Price Transparency Rule
The Hospital Price Transparency rule issued by CMS has been in effect since January 1, 2021. Since April, CMS has been issuing warning letters letting hospitals know about non-compliance with the rule, which can result in fines of up to $300 per day. CMS recently proposed an increase in the non-compliance penalty based on the number of beds, with the goal of further incentivizing hospitals to comply with the rule.
According to the CMS website, the price transparency rule requires two things: “a comprehensive machine-readable file with all items and services” and “a display of shoppable services in a consumer-friendly format”. The IHA team is available to provide guidance and assistance as Indiana hospitals continue working toward full compliance with this new rule.
 Governor Holcomb Signs HEA 1468 Dealing with Various Health Matters
Governor Holcomb Signs HEA 1468 Dealing with Various Health Matters
This week, the IHA team attended the bill signing ceremony for HEA 1468, authored by Representative Steve Davisson (R-Salem). IHA supported the legislation during session this year, in particular, due to the provisions the bill contains related to mental health and addiction treatment. The bill requires FSSA to apply for a Medicaid state plan amendment for reimbursement of Medicaid rehabilitation option (MRO) services for eligible recipients of certain services in a community mental health center and for reimbursement of MRO services concurrent with residential addiction treatment reimbursement. The legislation also specifies that telehealth services satisfy any face-to-face meeting requirement between a clinician and a consumer for purposes of a community mental health center. The bill went into effect on July 1, 2021
 Representative Davisson Receives Sagamore of the Wabash Award
Representative Davisson Receives Sagamore of the Wabash Award
Following the ceremonial bill signing, Governor Holcomb presented Representative Davisson (R-Salem) with a Sagamore of the Wabash award for his outstanding service to the state of Indiana. The Sagamore award is Indiana’s highest honor and is conferred upon deserving recipients at the Governor’s discretion. Representative Davisson has worked tirelessly to serve Indiana throughout his career as a state legislator, and as a pharmacist in Southern Indiana. IHA applauds the conferral of this award and joins with Governor Holcomb in expressing our appreciation for everything Representative Davisson has done to champion common-sense health care policies and protect the rights of Hoosiers.
Congratulations, Representative Davisson!
Legislative Update - August 5, 2021
Interim Study Committee Reviews Indiana’s Trauma System
This week, the Interim Committee on Public Health, Behavioral Health, and Human Services chaired by Senator Ed Charbonneau (R-Valparaiso), convened to examine Indiana’s trauma system including pre-hospital, hospital, and post-acute care settings. The committee received testimony from regulatory agencies and stakeholders on the current state of Indiana’s trauma and EMS systems. The goal of the committee is to improve equity in the system for all Hoosiers regardless of location and to consider enhancements in governance to improve outcomes. The committee will have two more meetings and will submit a report to the Legislative Council with any recommendations. More information about this committee can be found here.
Study Committee Examines License Reciprocity in Indiana
The Interim Committee on Public Policy, chaired by Senator Ron Alting (R-Lafayette), met today to discuss the advantages and disadvantages of professional licensing reciprocity, comparing Indiana with other states that allow reciprocity, including all of Indiana’s surrounding states. IHA testified in support of license reciprocity, emphasizing the pandemic’s devastating impact on Indiana’s pre-existing health care professional shortage and the urgent need to bolster the state’s workforce. The committee will meet again later this month and will submit a report to the Legislative Council with any recommendations. Click here to find more information on this committee.
IHA Promotes Trent Fox to Vice President of Government Relations
IHA is pleased to announce the promotion of Trent Fox to Vice President of Government Relations. Fox previously served as the association’s Senior Director of Public Policy and Legislative Relations. “IHA has a long history of working with the Indiana General Assembly and other stakeholders on health care policy issues, and we are fortunate to have outstanding talent like Trent to carry on this tradition,” said IHA President Brian Tabor. “I have full confidence in IHA’s legislative team to represent our members and advocate for the health of all Hoosiers.”
Brian Tabor Appointed to APCD Advisory Council
During the 2021 legislative session, the Indiana General Assembly passed HEA 1402 creating the All Payer Claims Database (APCD) Advisory Council, an important step in developing an effective and meaningful tool for Hoosiers seeking health care pricing and quality information. This week, IHA President Brian Tabor was appointed to serve on Indiana’s APCD Advisory Council. The addition of Tabor to the Advisory Council will ensure hospitals are comprehensively represented and that consumers will benefit from Indiana’s APCD, once established. As states strive to achieve high-quality, affordable care while improving health metrics, states are increasingly using data from APCDs to improve transparency. Policymakers, health care providers, and other stakeholders recognize APCDs as a promising tool that can help achieve this objective.

